|
|
|
||||||||||||
Dissector Answers - Heart |
|||||||||||||
Learning Objectives:
Upon completion of this session, the student will be able to:
- Identify the structures traversed in sequence of blood flow. Relate the anatomy of the heart to its basic physiological function.
- Identify the structures found in each of the four chambers and consider their significance.
- Compare and contrast the anatomical characteristics right and left sides of the heart.
- Identify the arterial supply and venous drainage of the heart. Describe the electrical conduction system.
- Describe the sternocostal projections of the valves of the heart and identify their auscultation points.
Learning Objectives and Explanations:
1. Identify the structures traversed in sequence of blood flow. Relate the anatomy of the heart to its basic physiological function. (W&B 389-392, N212, N221, N224, TG4-19)2. Identify the structures found in each of the four chambers and consider their significance. (W&B 389-395, N214, N220A, N220B, N221A, N221B, N222, N223A, N223B, N224, TG4-25A, TG4-25C, TG4-26A, TG4-26B)This is one of those cases when a picture is definitely worth "a thousand words":
The basic physiological function of the heart is to mechanically pump blood through both of the body's circulatory loops. The human heart is really two different pumps - one for each circuit. The atria are like miniature "priming pumps", whose job it is to help fill the ventricles. The ventricles, then, are the "main pumps" that move blood around the body.
One key point relates to the origin/attachment of the myocardium (heart muscle) to the fibrous skeleton. The myocardium, in a way, forms loops around each chamber, starting and ending at the fibrous skeleton. Therefore, when the muscle contracts, the chambers get smaller, squeezing the blood out of the heart.
3. Compare and contrast the anatomical characteristics of the right and left sides of the heart. (W&B 389-392, N220A, N220B, N221A, N221B, TG4-25A, TG4-25C, TG4-26A, TG4-26B)
- Right Atrium:
- sinus venarum: thin-walled posterior part, where vena cava empty (Latin, sinus = fold, hollow)
- pectinate muscle: muscular anterior part (Latin, pecten = comb)
- right AV (tricuspid) valve - superior surface: opens into right ventricle
- sulcus terminalis: external demarcation of separation of sinus venarum and pectinate muscle (Latin/Greek, holkos (sulcus)= furrow)
- crista terminalis: internal demarcation of separation of sinus venarum and pectinate muscle (Latin, crista = crest)
- opening of coronary sinus: this venous trunk drains most of the heart and dumps right into the right atrium (Latin, sinus = fold, hollow)
- fossa ovalis: remnant of foramen ovale, an opening in the interatrial septum in fetus (Latin, fossa = ditch, Latin, ovale = oval)
- Right Ventricle:
- conus arteriosis: smooth portion leading to pulmonary valve and trunk
- trabeculae carnae: ridged muscular wall (Latin, trabeculae = little beam, carnae = meaty)
- right AV (tricuspid) valve - inferior surface: opens from right atrium
- chordae tendinae: attach to cusps of AV valve, preventing both separation and prolapse (valves being pushed back into atrium) (Note: the chordae tendinae and papillary muscles do not "pull" the valves open.) (Latin, tendere = to stretch
- papillary muscles: contraction during systole (ventricular contraction) helps prevent valve prolapse and regurgitation of blood (Latin, papilla = nipple)
- pulmonary valve: leads to pulmonary trunk. Semilunar cusps prevent regurgitation of blood from pulmonary trunk during diastole (ventricular relaxation).
- Left Atrium:
- smooth-walled portion: no specific name, as in right atrium, but serves similar purpose - site of emptying of the four pulmonary veins
- pectinate muscle: muscular anterior part, near auricle (Latin, pecten = comb)
- interatrial septum: opening (closed at the other end by the fossa ovalis) to the right atrium (Latin, septum = partition, wall)
- left AV (mitral) valve - superior surface: opens to left ventricle (looks like a miter, the headdress worn by bishops)
- Left Ventricle:
- trabeculae carnae: ridged muscular wall (Latin, trabeculae = little beam, carnae = meaty)
- left AV (mitral, bicuspid) valve - inferior surface: opens from left atrium
- chordae tendinae: attach to cusps of AV valve, preventing both separation and prolapse (valves being pushed back into atrium) (Note: the chordae tendinae and papillary muscles do not "pull" the valves open.) (Latin, tendere = to stretch
- papillary muscles: contraction during systole (ventricular contraction) helps prevent valve prolapse and regurgitation of blood (Latin, papilla = nipple)
- aortic valve: leads to ascending aorta. Semilunar cusps prevent regurgitation of blood from ascending aorta during diastole (ventricular relaxation). (Greek, aorta = to lift)
4. Identify the arterial supply and venous drainage of the heart. Describe the electrical conduction system. (W&B 387-389, 396-397, N216A, N216B, N218, N219, N220, N222, N223, N225, TG4-23A, TG4-23B, TG4-23C, TG4-24B, TG4-24D, TG4-28A, TG4-28B)The right and left sides of the heart are very similar in terms of structural components. Both contain an AV valve, a semilunar outflow valve, smooth and muscular parts, etc. The primary difference between the right and left sides of the heart is size. The muscle of the left ventricle is 2-3 times thicker than that of the right, although the size of the cavity itself is about the same as the right. Both ventricles pump the same amount of blood, but the left ventricle must be much more powerful in order to perfuse the entire body, as opposed to the right ventricle that only has to perfuse the lungs. The systemic resistance to flow, which must be overcome by the left ventricle, is much higher than the pulmonary resistance to flow.
Arterial Supply:5. Describe the sternocostal projections of the valves of the heart and identify their auscultation points. (W&B 394 (clinical note), 380 (figure 5-23), N N212, N224, TG4-14)
Venous drainage:
The main vein of the heart is the coronary sinus. It receives blood from the great, middle, and small cardiac veins, the oblique vein of the left atrium, and the left posterior ventricular vein. The cardiac sinus, then, drains into the right atrium. Most of the anterior cardiac veins drain directly into the right atrium.
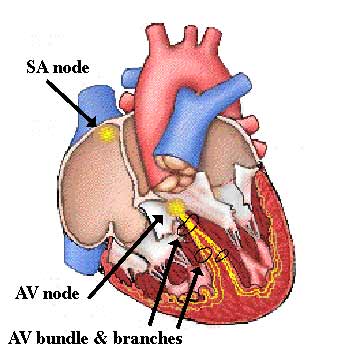
Electrical conduction:
The SA node is the "pacemaker" of the heart. It is located in the crista terminalis. It can generate signals independent of any CNS input, or it can be regulated by the autonomic nervous system.
The electrical signal travels from the SA node through the atrial myocardium, causing atrial contraction.
The signal then reaches the AV node, which is surrounded by the insulating fibrous skeleton. There is a significant delay here, to allow the ventricles to fill before they contract.
The signal leaves the AV node via the AV bundle, which splits at first into two branches, then into multiple branches to supply the ventricular myocardium. This splitting and quick conduction by the specialized cells of the bundle allow for all parts of the ventricle to contract together.
Due to location deep in the chest and/or directly behind the sternum, the sternocostal projections of the valves do not necessarily correspond to the best site of auscultation. In some cases, clinicians take advantage of the flow of blood through the valves, colliding with a spot on the muscular wall, to effectively auscultate.
Valve Sternocostal projection Point of auscultation Pulmonic left sternal border, 3rd rib 2nd, left IC space, just lateral to sternal angle Aortic left sternal border, 3rd IC space 2nd right IC space, just lateral to sternal angle Mitral left sternal border, 4th rib 5th, left IC space, 8cm lateral to midline Tricuspid midsternal, 4th IC space 4th, left IC space, just lateral to sternum The Loyola University Chicago - Stritch SOM website has very nice visuals for this concept here.
Cultural enrichment: Check out these sections from the 1918 version of Gray's Anatomy of the Human Body! Some of the terms are (of course) out-of-date, but the illustrations are timeless.The Heart - The Aorta - Surface Anatomy of the Thorax - Surface Markings of the Thorax
Questions and Answers:
6. Is the artery to the atrioventricular node a branch of the right, left, or both coronary arteries? (N216, N218, TG4-23B)In 80-85% of people, the artery to the AV node is a branch of the right coronary artery. It arises just before the RCA gives off the posterior interventricular branch.7. Define anterior cardiac and small cardiac veins. (N216, TG4-24B)Anterior cardiac veins: 3 or 4 small vessels arising on the anterior surface of the right ventricle. They cross the RCA (and the coronary sulcus) and end by penetrating the wall of the right atrium. Notably, most other veins drain into the coronary sinus rather than directly into the right atrium.8. Review the cardiac plexus and its distribution along the coronary vessels. (Latin, plectere = to braid) (N N126, N226, N227, TG8-14, TG8-15)
Small cardiac vein: usually begins as the marginal vein along the heart's acute margin. It receives tributaries from the right atrium and turns to the back of the heart, running with the RCA in the coronary sulcus. It ends by dumping into the right end of the coronary sinus.The cardiac plexus is a network of sympathetic and parasympathetic nerve fibers located in the concavity of the arch of the aorta and behind it on the trachial bifurcation (the superficial and deep plexuses respectively). The sympathetic nerves, which increase the rate and force of the heartbeat, arise from cervical and thoracic ganglia. The vagus nerve supplies the parasympathetic fibers, which act in opposition to the sympathetics.9. Define endocardium. (N221)The endocardium is the thin internal layer or lining membrane of the heart. It also covers the heart's valves.10. Examine the right atrioventricular (tricuspid) valve. Define the cusps. (N220, N222, N223, TG4-25A, TG4-25C, TG4-26A, TG4-26B)There are three cusps. The two larger ones are the anterior and the septal cusps. The smaller one is the posterior cusp.11. Define chamber walls: interventricular (or interatrial), anterior and posterior. (N220, N221, TG4-25A, TG4-25C, TG4-26A, TG4-26B)12. In the right ventricle, define papillary muscles, chordae tendinae, and tricuspid valve cusps. (Latin, papilla = nipple) (N220, TG4-25C)Right atrium: thin-walled sinus venarum posteriorly, more muscular anteriorly (including a muscular auricle), with interatrial septum between it and the left atrium
Left atrium: thin-walled portion posteriorly, muscular auricle more anteriorly, with interatrial septum between it and the right atrium
Right ventricle: lateral and anterior walls are muscular, while the posterior portion is mostly composed of interventricular septum
Left ventricle: interventricular septum is more anterior, rest of wall is muscular
The right ventricle usually has only two papillary muscles (anterior and posterior); occasionally there is one or more small septal papillary muscles. They are muscular projections from the ventricular wall which have tendinous cords (chordae tendinae) extending to the tricuspid valve cusps. The anterior muscle is the largest and has tendinous cords attaching to the anterior and posterior cusps. The smaller posterior muscle, which may consist of several parts, has cords attaching to the posterior and septal cusps. The septal muscle, when there is one, has cords attaching to the anterior and septal cusps. If there is no septal muscle, chordae tendinae arise directly from ventricle's septal wall.13. Do you find a septomarginal trabecula? (N220, TG4-25C)The septomarginal trabecula (moderator band), when present, is a muscular ridge of myocardium extending from the right ventricle's septal wall to the base of the anterior papillary muscle. (Latin, trabecula = little beam)14. Name the semilunar cusps of the pulmonary valve. (N220, N222, TG4-25C)The pulmonary valve's three semilunar cusps are named according to their orientations: right, left and anterior.15. Does the left atrioventricular (mitral, bicuspid) valve have any commissural cusps? Note relation of anterior cusp to aortic wall. (N221A, N221B, N222A, N222B, N223A, N223B, TG4-26A)
Commissural cusps are small accessory cusps occurring between the named cusps (anterior and posterior). The anterior cusp of the mitral valve abuts and curves around the base of the aorta.16. What is the aortic vestibule? (N221, TG4-27B)The aortic vestibule is the superior portion of the left ventricle which leads into the root of the aorta.17. Name the semilunar cusps of the aortic valve. (N221A, N221B, N222A, N222B, N223A, N223B, TG4-27B, TG4-26C)The aortic valve's three cusps, like the pulmonary valve's, are named according to position: right, left and posterior. The right and left cusps are associated with the right and left coronary arteries. The posterior cusp is referred to as the "non-coronary cusp".18. Where are the sounds associated with each heart valve best heard with a stethoscope? (N212, N224, TG4-14, Objective 5 above)Mitral: 5th left intercostal space19. What are the fibrous rings? (N222)
Tricuspid: 4th left intercostal space
Pulmonary: left upper sternal border
Aortic: right upper sternal borderThere are four fibrous rings, one surrounding each valve. They are made of dense collagen and are part of the heart's fibrous skeleton. This skeleton is the point of attachment/insertion for cardiac muscle - the atrial muscle from above and the ventricular muscle from below.20. What is the relationship of the heart's fibrous skeleton to its conduction system? Why is this important? (N222, N225, TG4-28A, TG4-28B)The fibrous skeleton provides attachment for heart's myocardium and valves. Additionally, it serves as an electrical insulator between the atria and ventricles penetrated only by the conduction system. This ensures that there is a pause between the contraction of the atria (leading to ventricular filling) and the contraction of the ventricles (ventricular ejection or emptying).