|
|
Clinical Cases |
|
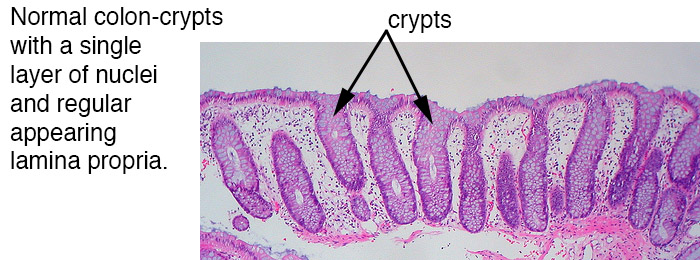
Colon cancer: Colorectal mucosa ranks third for most common site of cancer, and colorectal carcinoma causes the third most cancer-related deaths. The two categories of colon cancer are polypoid and non-polypoid. The subtypes of polyps are listed below:
- Hyperplastic - hyperplastic polyps are non-neoplastic, typically small, and are non-invasive.
- Hamartomatous - Hamartomatous describes a benign lesion of dysplastic growth of cells in their tissue of origin. This does not typically indicate an increased risk of malignancy. Polyps are non-neoplastic, typically small, and are non-invasive.
- Adenomatous - These polyps are pre-malignant lesions arising from the glandular tissue of the colon (adeno-), and can progress to carcinoma. The most common site of metastasis is the liver.
Image obtained from the Creative Commons database.
Hyperplastic - can see structures protruding into the lumen of crypts, forming a "saw tooth" appearance on histology.
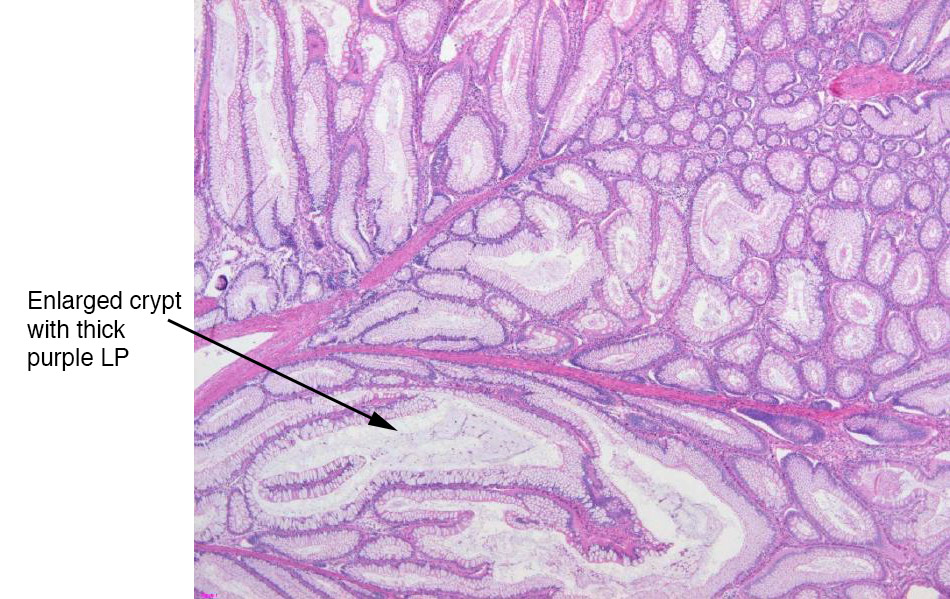
Hamartomatous - neoplasm resembles tissue of origin, featuring crypts and lamina propria. However, the structures are disordered, appearing as dilated crypts and/or increased area of the lamina propria. These lesions are benign, so the neoplasm is confined within the polyp.
Image obtained from the Creative Commons database.
Image obtained from the Creative Commons database.
Adenomatous - nuclear stratification. In this image, the adenomatous mucosa is on the left, and normal colonic tissue can be seen on the right.
Image obtained from the Creative Commons database.
Risk factors associated with development of colorectal cancer include family history, presence of adenomatous or serrated polyps, irritable bowel disease, tobacco use, and a diet low in fiber and high in processed meats. Patients often present with iron-deficiency anemia due to chronic GI bleeding. Colonoscopies and fecal occult blood tests are routinely performed on patients over 50 years of age in hopes of early detection.
Pathogenesis: There are two major pathways suspected to be at play in the development of colorectal cancer.
- Chromosomal instability pathway - mutations in the APC gene (a known tumor suppressor), can increase risk of colorectal cancer and FAP (familial adenomatous polyposis). This leads us to the "two-hit hypothesis," or loss of heterozygosity, which means that losing both APC alleles causes complete loss of function of tumor suppression activity from that gene product. FAP typically arises after puberty and patients present with thousands of polyps throughout the colon, always involving the rectum. These patients must receive a complete colectomy.
- Microsatellite instability pathway - This describes either mutations or methylations (silencing) of mismatch repair genes, especially MLH1. DNA mismatch repair is responsible for correcting mistakes made during DNA replication. The process involves recognizing erroneous base pairings, recognizing the daughter strand, and excising and replacing the erroneous base. Loss of this system exposes the cells to increased rates of uncorrected mutations and increases risk for sporadic colorectal cancer development.
The general cascade of mutations for development of colorectal cancer are as follows: 1) Loss of APC gene (tumor suppressor), 2) activating mutation of KRAS (an oncogene), and loss of p53 (tumor suppressor). Each step in this cascade exposes the colon to an increased risk of dysplastic process. After loss of p53 the colon is at highest risk of developing carcinoma.
Image obtained from the Creative Commons database.