|
|
Clinical Cases |
|
Nephrolithiasis
Nephrolithiasis (kidney stone formation) is a common condition with a lifetime prevalence of 10% in men and 5% in women. Kidney stones (nephroliths) are crystal aggregates of dissolved urinary minerals that form in the kidneys due to some abnormality in renal physiology and/ or urine content. When the urine becomes too concentrated with a certain mineral or combination of minerals, then it is possible for these dissolved substances to crystallize out of solution and form stones (renal calculi).
Because of the importance urine concentration has in stone formation, dehydration is the biggest risk factor for nephrolithiasis due to the subsequently high urine concentrations and low urinary output that result. There are several types of kidney stone, differentiated based on the primary mineral component of the stone:
- Calcium - The most common kidney stone is that formed primarily of calcium. These occur more commonly in men than women and persistently recur after they first appear between age 20-30. Calcium must bind with another substance to form the stone, and most frequently this substance is oxalate. It is thought that the main culprit in calcium oxalate stones is more oxalate than calcium (oxalate promotes stone formation 15x stronger than calcium, and calcium plays an important role in binding and clearing oxalate from the GI tract), which explains why diets low in calcium actually increase overall risk for developing kidney stones.
- Cystine - Cystine stones form in people with cystinuria, which is an autosomal recessive disorder that results in an inability to clear cystine from the urine.
- Uric acid - When uric acid accumulates in the bloodstream (a condition that leads to gout), or urine acidity remains excessively high (low urinary pH), uric acid tends to precipitate out of solution in the kidneys and form uric acid stones. This type of stone is commonly found in patients with gout and those patients on chemotherapy.
- Struvite - Struvite stones are commonly known as infection stones, and they require a more basic urine (higher pH) to form. Organisms like Proteus mirabilis are capable of metabolizing urea for energy within the urinary tract, resulting in the production of ammonia. When Proteus mirabilis causes a urinary tract infection (UTI), ammonia build-up increases the urinary pH, creating favorable conditions for the formation of struvite stones. Struvite stones are always associated with UTI, so if a stone is found and determined to be struvite, there must be a UTI present.
Knowing what type of stone a patient has is important in providing effective treatment, so clinicians often try to collect stones after they pass naturally or are surgically removed.
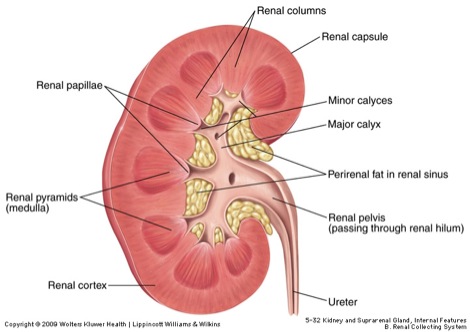
Kidney stones form in the major or minor calyces of the kidney or the renal pelvis, and can be found anywhere in the urinary tract downstream of these structures. Stones often become symptomatic only after passing from the renal pelvis into the ureters. Stones in the proximal ureter cause flank or upper abdominal pain, whereas those in the distal ureter can cause pain in the ipsilateral (same side) gonad. Once the stone reaches the junction of the ureter and bladder dysuria, polyuria, and hyperuria result, oftentimes being mistaken for a UTI.
Treatment
Treatment of acute stone events (obstruction/ passage through ureter or urethra) depends on the size of the stone. Most stones have a diameter of less than 5 mm and pass without intervention. For larger stones interventions such as lithotripsy (breaking a stone up using high intensity acoustic pulses), ureteroscopy (passing an endoscope through the urethra to access ureters, kidney stone can be visualized and removed via forceps using endoscope), or nephrolithotomy (surgical removal of stone through an incision in the back) can be utilized. Some clinicians will let a patient try and pass a stone up to 1 cm in diameter for 4 weeks before intervening, encouraging the patient to drink high volumes of water to increase urine flow and hasten the passage of the stone.
Many patients who have had a kidney stone will have another, as recurrence rates of nephrolithiasis are 30-50% within 5 years. Medical therapy and good hydration are the principle means of preventing chronic nephrolithiasis. The type of medical therapy utilized depends on the type of stone begin formed by the patient.
Diagnosis
The diagnostic gold standard for kidney stones is axial CT scan (CAT) without contrast (the same type of scan we have on all of our cadavers). Recent studies have shown CT scan to have a sensitivity of 98%, specificity of 100%, positive predictive value of 100%, and negative predictive value of 97% when being used to diagnose urolithiasis (stone formation anywhere in the urinary tract). In order to determine from CT scan whether a patient has a kidney stone, we must first be able to follow the urinary tract on CT from kidney to urethral meatus. Begin by looking at the anterior view of the urinary tract below. Notice that the kidneys can be found around the T11- L4 levels, and that the right kidney is often pushed inferior to the left kidney by the liver. The ureters come out of the kidney's hilum medially and run anterior to the psoas major, lateral to the inferior vena cava or abdominal aorta (depending on whether it's the right or left ureter). The bladder can then be found immediately posterior to the pubic symphysis. The urethra can be found by following the bladder inferiorly out to the urethral meatus of the penis or vagina.
The CT image below shows a patient with a kidney stone obstructing the proximal right ureter. Notice that we can tell the stone is in the proximal ureter because the level of the scan still includes the right kidney. The renal pelvis is just superior to the level of this cross-section.
Kidney Stone on CT ScanThe movie below is the CT scan of cadaver 33527. Begin by trying to follow the urinary tract of this patient from kidney to urethral meatus. The kidneys can be found in the retroperitoneum between the T12-L3 vertebrae (time 70-80, I11 and N11). Notice that the shape of these kidneys is C-shaped with the inward curve of the C facing medially. This is where the hilum of the kidney is, and it is where the renal pelvis and ureters will exit (as well as the renal artery and vein). Medial to the kidneys is the psoas major muscle (time 85, J9 and M9). It is important to find this muscle when looking for the ureters because the ureters ride right along the top of this muscle, lateral to the great abdominal vessels (IVC and abdominal aorta), until they reach the pelvis. You can catch the ureters coming out of the renal hilum just inferior to the renal artery and vein, so look first for the renal artery and vein (time 75, J9 and N9), then look closely at the cross-sections directly inferior to these vessels and you will find the tiny ureters (time 78, N9.5). The ureters are especially difficult to find because they are very small on CT scan, but spend some time looking between the kidneys and psoas major mm., and further inferior between psoas major and the IVC or abdominal aorta. Of course, the presence of a renal calculus would make the ureter much easier to be seen. The bladder can be found just posterior to the pubic symphysis, though on this patient the majority of the bladder is superior to the pubis (time 89-97, L8). Follow the bladder down through successively inferior cross-sections to find the urethra, which passes beneath the pubic symphysis and out through the penis (time 105, L6).
To find this patient's kidney stone, move the scan back up to the level of the kidneys. Look closely at the right kidney and see if you can find a stone in one of the major or minor calyces. The stone is small and still located proximally to the ureters, and so it was likely asymptomatic. The stone is located at time 76-77, I10.