|
|
Clinical Cases |
|
Vesicocutaneous Fistula
A fistula is defined as an abnormal connection or passageway between two organs or one organ and the body's exterior. A vesicocutaneous fistula, therefore, is an abnormally formed connection between the bladder (vesico-) and the exterior surface of the body (-cutaneous). These fistulas form secondary to surgery or trauma, and most commonly result from a suprapubic cystostomy site that fails to close.
Suprapubic Cystostomy
Also known as a vesicostomy or epicystostomy, the suprapubic cystostomy is a surgical procedure that creates a connection between the bladder and the skin so that patients with obstructed urinary outflow can drain their bladders. Patients who receive suprapubic catheters (via the cystostomy) usually have their urinary flow blocked by advanced BPH (benign prostatic hypertrophy), traumatic disruption of the urethra, congenital defects of the urinary tract, kidney stones, or a cancerous mass. Patients with spinal cord injuries also receive suprapubic catheters when intermittent urethral catheterization is no longer an option.
The cystostomy is maintained by placing a catheter through the surgical incision that connects the bladder and abdominal wall. This catheter is kept in place for up to a month as scar tissue forms around the catheter, forming a tract (a lumen) between the bladder and exterior abdominal surface. After formation of the tract is complete, the catheter can be removed periodically to help prevent infections, without losing the tract through which urine will be drained. Once the bladder no longer needs to be drained through the ostomy site, the catheter is permanently removed and the tract closes with time. Sometimes, however, the tract fails to close and a vesicocutaneous fistula results.
Suprapubic Cystostomy Technique
(courtesy of www.atlasofpelvicsurgery.com)
The procedure for placing a suprapubic catheter begins with the insertion of a forceps known as Randall Stone forceps through the urethral meatus and up into the bladder. The forceps is then used to push up on the abdomen above the pubic symphysis, providing a target for incision.
Upward pressure is maintained on the forceps while the tip of the forceps is palpated with a finger. Once the forceps have been palpated, a small suprapubic incision is made through the abdominal wall and overlying fascia until the forceps can be felt on the scalpel blade.
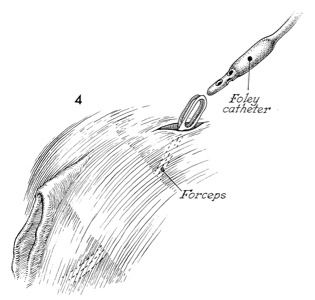
The forceps are forcefully pushed upward through the incision, where they can be used to grasp the tip of a Foley catheter.
The catheter is pulled into the bladder and the forceps are removed from the urethral meatus just prior to inflating the catheter balloon. After the catheter balloon is inflated and seated well inside the bladder, a sterile dressing is applied and the catheter is connected to a drainage bag.
Another type of vesicocutaneous fistula is the urachal fistula. This occurs when the urachus (the remnant of the allantois, which is the canal that drains the bladder of the fetus as it runs with the umbilical cord) fails to close after birth. Urachal fistulas are typically diagnosed after parents bring their infant to a pediatrician because urine is coming out of his/ her navel, and are therefore highly unlikely to be found in adult.
Vesicocutaneous Fistula on CT Scan
The movie file below is the CT scan of cadaver 33515. Scan down to the level of the bladder (time 90-95, I8-9). Notice that a fistula is seen extending from the bladder to the anterior abdominal surface. Scan slightly inferior to the fistula to see a few renal calculi (kidney stones) in the bladder (time 92-93, I10). It is possible that this patient's kidney stones warranted the placement of a suprapubic catheter, and that a vesicocutaneous fistula resulted from the failure of this ostomy site to close.