|
|
|
||||||||||||
Dissector Answers - Joints of the Lower Limb |
|||||||||||||
Learning Objectives and Explanations:
1. List and describe the various types of moveable joints and give examples of each type. (W&B 46-51, M 21-26)The three major types of joints, along with subtypes and examples, are listed here:2. List the characteristics of and identify the parts of a typical synovial joint. (W&B 47-49, M 23-26)
- Fibrous joints: the most simple joints. They are only connected by fibrous ligaments. A suture is a fibrous joint that eventually fuses, forming one bone from two (a synostosis), like in the skull of a growing infant. A gomphosis is the joint between a tooth and the jaw. A syndesmosis is a fibrous membrane or ligament that joints two bones. The tibia and fibula have an interosseous ligaments or membrane, as do the radius and ulna.
- Cartilaginous joints: joined by cartilage only. These joints are avascular or anervous, except at their margins. Synchondroses are temporary joints present in growing bones. The epiphyseal plate (growth plate) will later ossify into solid bone. The epiphysis has hyaline cartilage and the extension of ossification from the diaphysis side converts it to bone. A symphysis is a permanent cartilaginous union. They always have hyaline cartilage on the bony surfaces concerned, and these cartilaginous surfaces are joined by fibrous tissue or fibrocartilage.
- Synovial joints: "diarthroses" (freely moveable joints). These joints are joined by a fluid-filled capsule and accessory ligaments. Examples include the knee, ankle, and hip.
Synovial joints consist of:3. Recall the movement characteristics of the various types of synovial joints. (W&B 47-49, M 23-26)Types of synovial joints
- Hyaline cartilage: covers the full weight-bearing surface, providing a smooth yet resilient surface
- Joint capsule: a cavity, made of accessory ligaments, with synovial fluid inside. This reinforces the synovial membrane.
- Synovial membrane lining: secretes synovial fluid and covers the synovial cavity. It reaches to the edges of the hyaline cartilage.
- Accessory structures: accessory ligaments ("intracapsular" and "extracapsular"); articular discs or menisci, which are pads of fibrous cartilage; muscles and tendons; and subsynovial fat.
- Plane: involves flat surfaces. Movements consist of sliding of one surface on the other, and may be multidirectional in one plane. Examples: facet joints, joints of the tarsal bones of foot.
- Hinge (ginglymus): movement around a single axis at right angles to the bone. Permits flexion and extension only. These usually have strong collateral ligaments on each side reinforcing the joint. Examples: elbow, knee.
- Pivot (trochoid): rotary movement around a longitudinal axis. Rounded process of bone rotates within a sleeve or ring composed of a bony fossa and a strong ligamentous band. Examples: atlas-axis, radioulnar joint.
- Condyloid: oval surfaces allowing movements in two planes at right angles to each other. Example: radiocarpal joint
- Saddle (sellar): movement in two basic axes, with circumduction. Example: carpal-metacarpal joint of the thumb.
- Ball and socket: allows movement in any axis. Examples: hip, shoulder.
See #2 above.4. Describe the structure of the joints of the lower limb and the functional capabilities and limitations of each based on their bony structure and ligaments. (W&B 633-640, 642-644, M 607-613, 617-625, 632-635)5. Describe the blood and nerve supply of the joints and in particular the effect of interruption of blood to the head and neck of the femur. (W&B 634, 640, M 613-614, 626, 636)
Images from "Anatomy of the Human Body" by Henry Gray are provided by:
The hip joint is a ball and socket type of joint. The femoral head is the ball, while the acetabulum is the socket. It is the second most movable joint in the body, with only the shoulder having greater range of motion. This joint is not only flexible, but strong by necessity. During standing, the entire weight of the body is transferred to the head and neck of the femur. The acetabular labrum helps provide this strength by grasping more than half of the head of the femur. (Latin, acetabulum = vinegar cup) The main ligaments of the hip joint are really thickenings of the fibrous capsule, which is attached to the acetabulum and transverse acetabular ligament. Some deep fibers pass circularly around the neck forming the zona orbicularus. These fibers form a collar around the neck that constricts the capsule and helps hold the femoral head in the acetabulum. This fibrous capsule does not attach to the posterior aspect of the femur. (This creates a possibility for dislocation backward, say, if your knees hit the dashboard of a car that, with the assistance of a tree, makes a sudden stop.) As the thigh becomes fully extended, the capsule is twisted and shortened, and the head of the femur is guided like a screw into its socket. Stability is at a maximum with hyperextension and at a minimum with flexion. (That is another reason why the femur gets pushed posteriorly with a car accident. The victim is sitting with the hip in a flexed, less stable position.) The four ligaments of the joint, listed below, allow considerable flexion of the hip joint, but restrict extension of the joint to 10 to 20 degrees beyond the vertical position.
- iliofemoral ligament: Y-shaped. It prevents hyperextension of the hip joint during standing by screwing the femoral head into the acetabulum.
- pubofemoral ligament: prevents overabduction of the hip joint.
- ischiofemoral ligament: It also screws the femoral head medially into the acetabulum, preventing hyperextension of the hip joint. This ligament also forms the posterior free margin of the capsule.
- ligament of the head of the femur: weak and of little importance in strengthening the hip joint.
Images from "Anatomy of the Human Body" by Henry Gray are provided by:
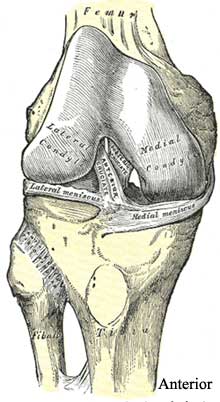
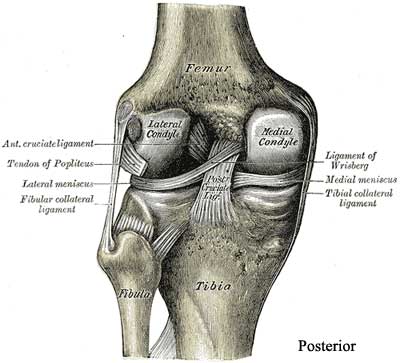
The knee joint is basically a hinge type of joint, allowing flexion and extension. The hinge movements are combined with some gliding and rolling and with some rotation about a vertical axis. This allows free motion in one primary plane combined with decent stability. The fibrous capsule is deficient in a few areas to allow tendons to pass through to the outside. The synovial membrane lines the fibrous capsule and attaches to the periphery of the patella and the edges of the menisci. (Latin, patella = shallow dish, Greek, meniskos = moon, crescent). It reflects onto the cruciate ligaments and also reflects between the tibia and fibula, covering the infrapatellar fat pad. This technically separates the fat pad and the cruciate ligaments from the joint cavity. The knee joint is relatively weak and depends on several things to strengthen it. First, its area of weight distribution is two or three times larger than either the tibia or the femur, which reduces the overall pressure. Furthermore, a strong fibrous capsule, the medial patellar and lateral patellar retinacula, patellar tendon, iliotibial tract (lateral side), and longitudinal fibers of fascia lata (medial side) all serve to strengthen the joint. Finally, two groups of important ligaments help add stability:collateral ligaments: capsular and extracapsular. They become taut in extension and prevent hyperextension, also prevent abduction and adduction. The medial collateral ligament, at its midpoint, firmly attaches to the medial meniscus. It is the weaker of the two, so injuries are more common here and, moreover, will usually involve the medial meniscus. The lateral collateral ligament is separated from the lateral meniscus by the tendon of the popliteus. Other extracapsular ligaments that strengthen the knee are the patellar ligament, the oblique popliteal ligament and the arcuate popliteal ligament.
cruciate ligaments: intracapsular. The anterior cruciate ligament (ACL) is weaker than the posterior cruciate ligament (PCL). They both prevent movement of the tibia forward or backward under the femoral condyles. They become taut in all positions of flexion but mostly with full extension and full flexion. (cruciate = cross-shaped)
Images from "Anatomy of the Human Body" by Henry Gray are provided by:
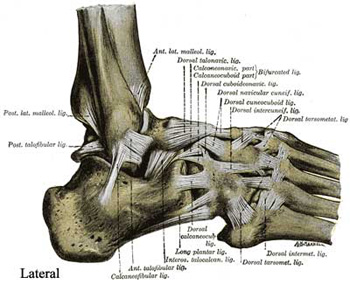
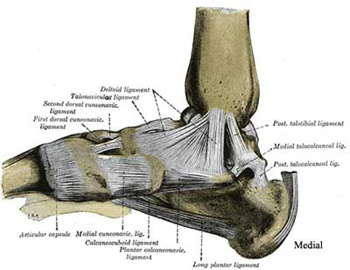
The ankle joint is a hinge type of synovial joint. It is located between the distal ends of the tibia and fibula and the superior part of the talus. The distal ends of the tibia and fibula form a deep socket into which the trochlea of the talus fits. (Latin, trochlea = block of pulleys, from Greek, trochos = wheel) The tibia itself articulates with the talus in two places: the inferior surface and medial malleolus of the tibia. The medial malleolus grips the talus tightly during movements of the joint. This grip is strongest during dorsiflexion because the anterior part of the talus is wider than the posterior, and that wide section is forced into the joint. Plantar flexion is relatively unstable and most injuries occur then. The lateral malleolus of the fibula also articulates with the talus. The ankle joint has less range of movement than the knee or the hip, so there are fewer supporting structures needed. The fibrous capsule is supported on each side by strong collateral ligaments The lateral ligament is composed of three parts:The medial ligament has four parts, but you only need to know it as the deltoid ligament. It stabilizes the ankle during eversion and prevents subluxation (partial dislocation) of the joint. (deltoid = shaped like a delta... the Greek letter)
- anterior talofibular ligament: a flat, weak band
- posterior talofibular ligament: a thick, fairly strong band
- calcaneofibular ligament: a round cord
6. Identify and describe the structure and function of the knee joint and in particular the effects of injury to the ligaments and menisci. (W&B 635-641, M 617-630)
- Hip:
- Blood Supply:
- medial and lateral circumflex femoral arteries: these are usually branches of the deep femoral artery, but sometimes they are branches of the femoral artery itself. The medial branch supplies the most blood.
- artery to the head of the femur: a branch of obturator artery. It enters the joint through the ligament of the head of the femur.
- Nerve Supply:
- femoral nerve and branches: anteriorly
- accessory obturator nerve: if present, anteriorly
- obturator nerve, anterior division: inferiorly
- superior gluteal nerve: superiorly and posteriorly
- nerve to quadratus femoris: posteriorly
- Knee:
- Blood Supply:
- genicular branches of femoral artery: contribute to genicular anastomosis
- popliteal branches, anterior recurrent, and posterior recurrent branches of the anterior tibial recurrent and circumflex fibular arteries: contribute to genicular anastomosis
- middle genicular branches of popliteal artery: penetrate the fibrous capsule of the knee joint and supply the cruciate ligaments, synovial membrane, and peripheral margins of the menisci
- Nerve Supply: branches of the obturator, femoral, tibial and common fibular nerve
- Ankle:
- Blood Supply: derived from malleolar branches of the fibular artery and the anterior and posterior tibial arteries
- Nerve supply: derived from the tibial nerve and the deep fibular nerve
The structure and function have been described in #4 above. The possibilities for injury are numerous and often serious. The knee's stability depends almost entirely on its associated ligaments and muscles, yet it must still be mobile, making it very prone to injury. Below are the most common injuries:7. Identify the structure of the ankle and foot joints and describe how the joints and ligaments provide firm footing but flexibility of movement. (W&B 642-652, M 632-645)
- tibial collateral ligament: caused by a blow to the lateral side of the knee. Since the tibial collateral ligament is firmly attached to the medial meniscus, tearing it frequently results in concomitant tearing of the meniscus. Furthermore, in many cases there is also trauma to the ACL, resulting in the "terrible triad", which is common in football.
- medial meniscus: can also be damaged independently by "twisting strains". (The lateral meniscus is hardly ever injured.) Small tears will heal themselves, but if the tear is large enough, the torn part of the meniscus can be removed with no loss of mobility. However, the tibial plateaus often undergo inflammation. These injuries are especially common in football and volleyball.
- anterior cruciate ligament: severe force to the anterior knee can cause a tear of the ACL. This causes the tibia to be able to slide anteriorly from the femur, which is diagnostic as the "anterior drawer sign". Skiing accidents are an example of a frequent cause of ACL tears.
- posterior cruciate ligament: ruptures when a player lands on the tibial tuberosity with the knee flexed. This is usually in conjunction with tibial or fibular collateral ligament tears. It is diagnosed with the "posterior drawer sign". These injuries are pretty common in basketball, and can also happen in head-on collisions when seatbelts are not worn.
The structure of the ankle joints have been described in #4 above. The following are the structures of the foot joints, as described in the session on the foot:8. Describe the arches of the foot and how the bony structure and ligaments form and support them.
Joints:
The subtalar joint is formed between the large concave facet on the under surface of the body of the talus and the convex posterior articular surface on the superior aspect of the calcaneus. A loose, thin walled articular capsule unites the two bones by attaching to the margins of the articular surfaces. This joint allows the foot to be placed firmly on slanting and irregular surfaces.The transverse tarsal joint is the designation for the irregular plane which extends from side to side across the foot and is composed of the talonavicular articulation medially and the calcaneocuboid joint laterally. This joint allows inversion and eversion of the foot.
Ligaments:
The plantar ligaments of the joints of the foot are very strong. They they are supplemented by robust interosseous ligaments which keep the bones from spreading apart. Notable on the sole of the foot are the long plantar ligament and the plantar calcaneocuboid and plantar calcaneonavicular ligaments. The elasticity of the latter and its support of the head of the talus have led to it being called the "spring ligament." The plantar aponeurosis may be likened to a "tie rod" for the longitudinal arch, firmly connecting its ends and preventing their spread.There are two longitudinal arches, medial and lateral. They pass from the calcaneus to the talus to the navicular to the cuneiforms to the metatarsals. They are supported by the plantar calcaneonavicular ligament (spring ligament), and also by the tendons of the tibialis anterior and tibialis posterior muscles. The transverse arch results from the shape of the distal row of tarsal bones and the bases of the metatarsal bones. Imagine an arch that goes over the top of the cuneiforms and cuboid, and is supported by the shape of the bones, various ligaments, and the tendons of the fibularis longus, tibialis anterior, and tibialis posterior muscles.
Cultural enrichment: Check out these sections from the 1918 version of Gray's Anatomy of the Human Body! Some of the terms are (of course) out-of-date, but the illustrations are timeless. Classification of Joints - The Kind of Movement Admitted in Joints - Hip Joint - Knee Joint - Ankle Joint - Arches of Foot - Surface Anatomy of the Lower Extremity - Surface Markings of the Lower Extremity
Questions and Answers:
9. What contacts the articular (medial) surface of the lateral malleolus?The medial side of the lateral malleolus, which is part of the fibula, articulates with the lateral surface of the talus.10. Note the iliopectineal bursa beneath the iliopsoas. Does it communicate with the hip joint?The iliopectineal bursa lies between the iliopsoas muscle and the capsule. When the capsule is perforated here, the bursa is open to the joint cavity.11. Trace the obturator externus tendon beneath the neck of the femur into the trochanteric fossa. What is its action and innervation?The obturator externus muscle is involved in lateral rotation of the thigh, as is the obturator internus muscle. It also stabilizes the head of the femur. The obturator externus muscle is innervated by the obturator nerve.12. What is the importance of the blood supply to the articulations involving the zona orbicularis, the acetabular labrum, the transverse ligament and the ligamentum capitis femoris (ligament of the head of the femur)?There is no collateral supply really available for the head of the femur or the parts around it. The main blood supply comes from the lateral, and especially the medial, circumflex femoral arteries. If the medial circumflex femoral artery is damaged, the small artery of the ligament of the head is not sufficient, and avascular necrosis of the femoral head will occur.13. What is the difference between the two collateral ligaments in the knee joint?The lateral is stronger and does not attach to the meniscus, while the medial is weaker and does attach to the meniscus.14. What is the function of the patella?The patella is a large sesamoid bone that developed in the tendon of the quadriceps femoris muscle. It pushes against the anterior articular surface of the femur's inferior surface, and, by holding the tendon off the lower end of the femur, improves the angle of approach of the tendon to the tibial tuberosity.15. With what does the patella articulate?See above #14 above.16. What are the actions of the cruciate ligaments?They stabilize the knee joint by preventing the movement of the tibia forward or backward, with the anterior cruciate ligament preventing anterior displacement and the posterior cruciate ligament preventing posterior displacement.17. What are the "drawer sign" and the "terrible triad"?The anterior drawer sign, movement of the tibia anteriorly when the flexed leg is pulled anteriorly, indicates anterior cruciate ligament rupture. The posterior drawer sign, movement of the tibia posteriorly when the flexed leg is pushed, indicates posterior cruciate rupture. The terrible triad is a tearing of the medial collateral ligament, the medial meniscus, and the anterior cruciate ligament all at the same time.18. What does the transverse tibiofibular ligament do?This ligament helps to hold tibia and fibula together. It also forms a portion of the articulation with talus.18a. Relate the arrangements of the malleoli and ligaments to the prevalence of ankle sprains.Most ankle sprains are caused by inversion of the foot, which causes tearing of the lateral ligaments: the calcaneofibular and posterior talofibular ligaments. Slight sprains might involve just partial tears, such as in the anterior talofibular ligament. Sometimes the lateral malleolus can be avulsed off the fibula or the fibula fractured if the ligaments are particularly strong. In effect, the ligaments are stronger than the bone, and the bone often "gives" first. The medial ligament is more rarely strained, but when it is it is due to eversion of the foot.19. How is the stability of the ankle joint provided?See #4 and #7 above.20. Which position is most stable? Why this position?Dorsiflexion is more stable than plantarflexion. The talus is stabilized due to the wider anterior side of the trochlea being immobilized by the tibial articulation. In plantarflexion, the skinnier posterior side is articulating more and so more movement is possible since it does not completely fill the space allowed the anterior side.21. What muscles provide action of the ankle joint?Dorsiflexion: muscles of anterior compartment of leg. These include the tibialis anterior muscle, the extensor hallucis longus muscle, the extensor digitorum longus muscle, and the fibularis tertius muscle. When the foot is fully everted, it is also fully dorsiflexed. (But remember, inversion and eversion are actions of the foot itself.22. What muscles provide stability of the ankle joint?
Plantarflexion: muscles of posterior compartment of leg. These include the tibialis posterior muscle, the flexor hallucis longus muscle, the flexor digitorum longus muscle and the plantaris muscle. The lateral compartment also participates in plantar flexion. (In fact, all muscles which enter the foot behind the malleoli plantarflex the foot. When the foot is fully inverted, it is also fully plantarflexed.All of the muscles mentioned above that cross the ankle lend stability to the ankle. The ligaments provide the stability as well. See also #4 and #7 above.23. What is the function of the plantar ligaments dissected?long plantar ligament: maintains the arches of the foot and forms tunnel for the tendon of the fibularis longus by extending some its fibers to the bases of the metatarsals.24. What are the actions of the subtalar articulation?
short plantar ligament: deep to the long plantar ligament. It also provides support of the longitudinal arch.
plantar calcaneonavicular (spring) ligament: highly elastic. It completes the socket for the head of the talus bone on the medial side and provides springy cushion for the foot. It also helps maintain the longitudinal arch of the foot.This joint is pretty stiff, though it allows some inversion and eversion.25. What is the tarsal sinus?It is a cavity lying between the talus and the calcaneus.26. What is the interosseous talocalcaneal ligament?This ligament is located inside the tarsal sinus. It is a strong band which connects the adjacent surfaces of the talus and the calcaneus along the oblique tarsal grooves. It provides support for the subtalar joint.27. What are the two parts and the action of the transverse tarsal joint?It is formed by the combined talonavicular and calcaneocuboid joints. The two separate joints align transversely. (Transection across the transverse tarsal joint is a standard method for surgical amputation of the foot.)28. What are the actions of the foot?
Inversion and eversion take place primarily through the transverse tarsal joint.Dorsiflexion, plantar flexion, inversion and eversion of the foot are the main actions of the foot.