|
|
|
||||||||||||
Dissector Answers - Lungs and Mediastina |
|||||||||||||
Learning Objectives:
Upon completion of this session, the student will be able to:
- Identify the contents of the superior mediastinum.
- Identify and trace the tributaries to each of the brachiocephalic veins and the formation of the superior vena cava.
- Identify and trace all the branches of the arch of the aorta in the region and the relationship of the vagus and phrenic nerves to them.
- Identify the thoracic part of the trachea and describe its blood supply and innervation.
- Identify and describe the location of the lungs in the thoracic cavity.
- Identify the relations of the pulmonary artery, pulmonary veins, and the bronchi at the hilum of each lung.
- Define a bronchopulmonary segment and discuss its general organization.
- Name the bronchopulmonary segments and give their approximate location in reference to the lobes of the lungs.
- Trace the lymphatic drainage of the lungs and respiratory tract.
- Define the boundaries of the posterior mediastinum.
- Describe the major contents of the posterior mediastinum and their relationships.
- Describe the organization of the thoracic sympathetic trunk, in addition to its visceral and splanchnic branches.
Learning Objectives and Explanations:
1. Identify the contents of the superior mediastinum. (W&B 370, M 138, 142-150, N193, N206, N209, N211, N212, N232, N240, N262, TG4-18, TG4-35A, TG4-35B, TG4-36A, TG4-36B)2. Identify and trace the tributaries to each of the brachiocephalic veins and the formation of the superior vena cava. (W&B 384, N74, N238, TG4-37B)
- Vessels:
- Arch of the aorta and roots of major branches: begins at the level of the sternal angle and arches superoposteriorly (up and back) and to the left. The arch usually gives off three major branches (below) supplying the head, neck, and upper extremities. (Greek, aorta = to lift)
- Brachiocephalic trunk: first branch of the aortic arch. The brachiocephalic trunk rises superolaterally and splits into the right subclavian and the right common carotid arteries. (Latin, bracchium = arm, Latin/Greek, cephalicus/kephalikos = head)
- Left common carotid artery: second branch. It ascends into the neck to supply the left side of the head. (Greek, kara = head)
- Left subclavian artery: third branch. It ascends lateral to the left common carotid into the neck, but does not give off any branches in the mediastinum. ("clavian" refers to the clavicle)
- Brachiocephalic veins: formed by the joining of internal jugular and subclavian veins. The brachiocephalic veins drain the head and upper extremities, uniting to form the superior vena cava, which dumps into the right atrium. (Latin, bracchium = arm, Latin/Greek, cephalicus/kephalikos = head)
- Superior vena cava (upper portion): returns blood to the heart from the head, neck, upper extremities, and thorax (except the heart and lungs). The terminal SVC lies in the middle mediastinum.
- Thoracic duct: drains all of the lymph from all of the body below the diaphragm and the left half of the body above the diaphragm. In the superior mediastinum it can be found behind the aortic arch, on the left side of the esophagus.
- Nerves:
- Right vagus nerve (CN X): enters thorax anterior to the right subclavian artery, giving off the right recurrent laryngeal nerve (which hooks back up into the neck to supply the larynx). The right vagus nerve then travels in a posteroinferior direction, following the right side of the trachea. It contributes to the cardiac, pulmonary, and esophageal plexuses. (Latin, vagus = wandering, plectere = to braid)
- Left vagus nerve (CN X): descends into the mediastinum between the left common carotid artery and the left subclavian artery. It gives off the left recurrent laryngeal nerve, which is distinctive because it wraps around the aortic arch before it travels up into the neck to supply the larynx. The left vagus then travels posteroinferiorly, contributing to the cardiac, pulmonary, and esophageal plexuses. (Latin, vagus = wandering, plectere = to braid)
- Phrenic nerves: provide somatic motor and sensory innervation to the diaphragm. These nerves pass anterior to the roots of the lungs, which separates them from the vagus nerves which pass posterior to the roots of the lungs. Contribution to the phrenic nerves include the 3rd, 4th, and 5th cervical spinal nerves - "C3, 4, and 5 keep the diaphragm alive."
- Viscera/Fascia:
- Thymus: a primary lymphoid organ, Important in the immune system, the thymus is the site of T-cell differentiation. (Greek, thymus = warty excrescence)
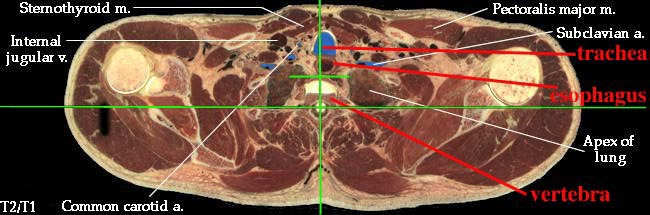
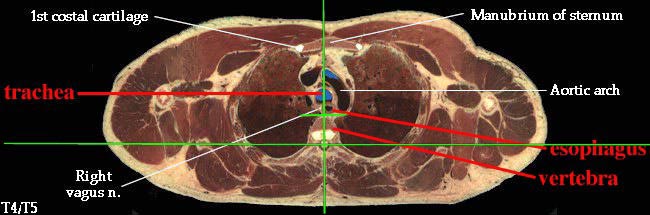
- Trachea: lies anterior to the esophagus, just a bit to the right of the median plane. The bifurcation into right and left main bronchi occurs at the level of the sternal angle. (Greek, trachys = rough)
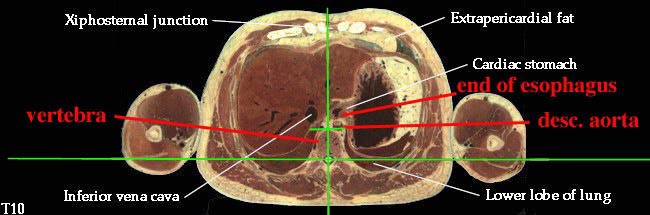
- Esophagus: enters the mediastinum a little to the right of the median plane, posterior to the trachea. It passes to the middle of the body, then to the left and anteriorly as it travels down to the stomach. (See "Extra Explanation" in Posterior Mediastinum Answers.) (Greek, oisein = to carry + phagein = to eat)
- Ligamentum arteriosum: remnant of fetal ductus arteriosus. The ligament attaches between the inferior surface of the aortic arch and the root of the left pulmonary artery. (Latin, ligare = band, tie)
3. Identify and trace all the branches of the arch of the aorta in the region and the relationship of the vagus and phrenic nerves to them. (W&B 383-384, N211, N212, N232, N237, N240, TG4-38)4. Identify the thoracic part of the trachea and describe its blood supply and innervation. (W&B 234-235, N33, N74, N126, N207, N209, N240, TG4-33, TG4-38)As discussed above, the arch of the aorta gives off the brachiocephalic artery (which splits into right common carotid and right subclavian arteries), the left common carotid artery, and the left subclavian artery. Also consider the veins of this region, which as a rule of thumb, lie anterior to the "analogous" artery.
Most laterally, we have the phrenic nerves. They lie on the anterior aspects of the anterior scalene muscles on both sides. These muscles separate the respective subclavian veins (anterior) from the subclavian arteries (posterior). So, the phrenic nerves cross between subclavian vein and subclavian artery as they descend into the thorax.
The vagus nerves are more medial, descending into the thorax just lateral to the common carotid arteries. They are also mostly anterior to the branches and the arch proper as they descend. The right vagus nerve gives off the right recurrent laryngeal nerve, which loops around to the posterior aspect of the right subclavian artery and travels back up into the neck. The left vagus nerve gives off the left recurrent laryngeal nerve, which loops around the arch proper, next to the ligamentum arteriosum, and ascends back into the neck between the trachea and the esophagus.
5. Identify and describe the location of the lungs in the thoracic cavity. (W&B 401-404, N196, N197, N199, N206, TG4-13A, TG4-13B, TG4-15, TG4-16, TG4-17, TG4-18)The trachea begins at the level of C6 and terminates at the level of the sternal angle, where it divides into the two main bronchi. The trachea receives arterial supply from the inferior thyroid arteries, internal thoracic arteries, and branches of the bronchial arteries. The blood drained via tracheal veins ends up in the inferior thyroid veins. Parasympathetic innervation to the smooth muscle and glands is via the vagus nerve (CN X), either directly or by the recurrent laryngeal nerves. Sympathetic innervation comes directly from the sympathetic trunk.
6. Identify the relations of the pulmonary artery, pulmonary veins, and the bronchi at the hilum of each lung. (W&B 400, N199, TG4-31AB, TG4-31CD, TG4-34A)The lungs occupy the large space inside the rib cage, on either side of the mediastinum, superior to the diaphragm. These spatial demarcations also define the three surfaces of each lung, namely the costal, mediastinal, and diaphragmatic surfaces. (The pleura of the same name covers the lung over that surface.) The lungs extend out of the thoracic cavity into the root of the neck at the apex, which is covered by the cervical pleura.
Each lung has a hilum on its medial aspect. The hilum of the lung is the point of entry for the root of the lung, which includes the bronchi, the pulmonary arteries, and the pulmonary veins. A pleural sleeve is created around these structures, where the pleura reflects, changing from visceral to parietal. Inferior to the hilum on each lung is the pulmonary ligament, a continuation of that pleural reflection.
7. Define a bronchopulmonary segment and discuss its general organization. (W&B 402, 404-407, N201, N203, N204, N205, TG4-32AB, TG4-32CD, TG4-33A)
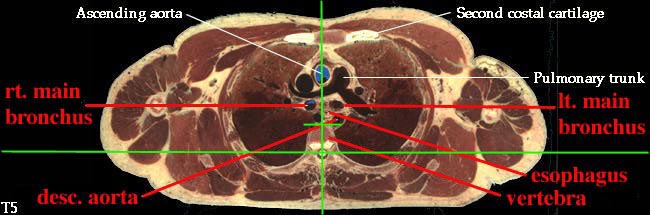
On both sides, the bronchus is posterior and the pulmonary vein(s) are anterior and inferior. The difference between the two involves the pulmonary artery(ies). On the right side, the artery(ies) lie more or less anterior to the bronchus. On the left side, however, the artery(ies) are the most superior structure, even superior to the bronchus.
8. Name the bronchopulmonary segments and give their approximate location in reference to the lobes of the lungs. (W&B 402, N201, N203, TG4-32AB, TG4-32CD, TG4-33A)A bronchopulmonary segment:
- is pyramid shaped, with the apex at the lung root;
- is the largest subdivision of a lobe;
- is surrounded by connective tissue;
- has separate arterial supply from other segments and receives its own segmental (tertiary) bronchus;
- is drained by intersegmental veins that lie in the connective tissue around the segment; and
- can be removed surgically without affecting the function of other segments.
Bronchi (gas exchange): Each segment is supplied by one tertiary bronchus (see below). This "conducting" bronchus branches about 15 times, the result of which is small "terminal" bronchioles. These terminal bronchioles branch several more times, becoming "respiratory" bronchioles, which have alveoli along them, allowing for some gas exchange. The terminal bronchioles terminate in several alveolar sacs, where most of the gas exchange takes place. (Latin, alveus = cavity, hollow)
Pulmonary arteries (deoxygenated blood): Leaving the right ventricle and traveling through the pulmonary arteries, the blood eventually reaches intrasegmental arteries. These arteries follow the branches of the bronchi and eventually end in capillary beds in the alveolar sacs. It is here that oxygen from the air crosses alveolar walls and enters the blood, while carbon dioxide from the blood goes the opposite way, to be exhaled from the lungs. It is important that you do not confuse pulmonary intrasegmental arteries with intrasegmental bronchial arteries. The former carry the deoxygenated blood from the right side of the heart in order to pick up oxygen. The latter are systemic, carrying oxygenated blood, like all systemic arteries, to supply the tissues of the bronchi.
Pulmonary veins (oxygenated blood): The pulmonary veins arise at the alveolar capillary beds and travel within the intersegmental septa to carry newly oxygenated blood back to the heart. These veins, as they begin to accept tributaries, will effectively drain both segments separated by the septa within which they run.
Right Lung:*
Superior Lobe: a three-piece lobe - a posterior and an anterior segment next to one another with an apical segment on top Middle Lobe: a flat, two-piece lobe that sits on the anterior aspect of the lung - a medial and a lateral segment next to one another Inferior Lobe: a five-piece, "square-based-pyramid" - four basal segments that point to the four "sides" of the body (anterior basal, medial basal, lateral basal, and posterior basal), and a superior segment on top. Left Lung:*
Superior Lobe: similar to the right superior lobe, except that the apical and posterior fuse to form an apicoposterior segment; there is also an anterior segment like on the right side. However, the left also has a "lingual" portion, with a superior and an inferior segment. Inferior Lobe: a five-piece, "square-based-pyramid" - four basal segments that point to the four "sides" of the body (anterior basal, medial basal, lateral basal, and posterior basal), and a superior segment on top. NOTE: the anterior and medial basal segments often fuse, resulting in an anteromedial basal segment in the left lower lobe.
9. Trace the lymphatic drainage of the lungs and respiratory tract. (W&B 234-235, N208, TG4-42)10. Define the boundaries of the posterior mediastinum. (W&B 370-371, N231, TG4-14)Lymph from the lungs drains first to pulmonary nodes, which are small nodes within the lung tissue and also beneath the visceral pleura. The numerous small pulmonary nodes drain into larger bronchopulmonary nodes located the hilum (also called hilar nodes). The bronchopulmonary nodes drain into tracheobronchial nodes located around the tracheal bifurcation. These nodes may be separated into three large groups. The large cluster of nodes below the tracheal bifurcation are called inferior tracheobronchial nodes (or carinal nodes) and they receive lymph from the lower lobes primarily. Beside the tracheal bifurcation on either side are the fairly large superior tracheobronchial nodes. Oddly, most of the lymph from the inferior tracheobronchial nodes drains up into the right superior tracheobronchial nodes, which means that lymph from the lower lobe of the left lung crosses to the right here, for the most part. The lymph drainage ascend beside the trachea, with several modest sized paratracheal nodes intercepting some of this lymph on either side. The lymph channels coalesce as they ascend to form bronchomediastinal lymph trunks on either side. The left bronchomediastinal lymph trunk drains into the termination of the thoracic duct in the root of the neck, and the right bronchomediastinal trunk usually unites with the right subclavian and right jugular lymph trunks to form a short right lymphatic duct, which drains, similar to the thoracic duct, into the junction of the subclavian and internal jugular veins on the right.
11. Describe the major contents of the posterior mediastinum and their relationships. (W&B 370, 408-416, N172, N192, N193, N194, N206, N207, N212, N232, N237, N238, N240, N260, TG4-35, TG4-35, TG4-36, TG4-36, TG4-37, TG4-37)
- Superior: plane b/w sternal angle and T4/T5
- Inferior: diaphragm
- Anterior: pericardium (middle mediastinum)
- Posterior: spinal column
- Vagus nerves (CN X):
- See Objective #1 above.
- Descending aorta (thoracic portion): the continuation of the arch of the aorta, supplying oxygenated blood to thorax (except the heart), abdomen, pelvic region, and lower extremities. It begins on the left side, but moves to the midline (to lie on vertebrae) as it descends. The branches of the thoracic descending aorta include:
- bronchial arteries - supplying the lower trachea and bronchial tree
- pericardial arteries - supplying the pericardium
- posterior intercostal arteries - supplying the intercostal muscles, spinal cord and vertebral column, deep back muscles, and the skin and superficial fascia overlying the intercostal spaces
- superior phrenic arteries - supplying the diaphragm
- esophageal arteries - supplying the lower 2/3 of the esophagus
- mediastinal arteries - supplying the lymph nodes and tissues of the posterior mediastinum
- subcostal arteries - supplying the vertebrae, spinal cord and muscles, skin, and fascia of the upper abdominal wall. They are just like intercostal arteries, but occur below the 12th rib.
Once the thoracic aorta goes through the aortic hiatus in the diaphragm, its name changes to abdominal aorta.
- Esophagus: enters the mediastinum a little to the right of the median plane, posterior to the trachea. It passes to the middle of the body, then to the left and anteriorly as it travels down to the stomach. (See "Extra Explanation" below.)
- Azygos vein system: serves to drain the back, the walls of the thorax and abdomen, and the mediastinal viscera. Although there is a great deal of variation, the usual arrangement is thus (W&B 411-412):
- azygos vein: runs up the right side of the vertebrae, arching over the root of the right lung to join the superior vena cava. The azygos receives blood from the right posterior intercostal veins, as well as the hemiazygos and accessory hemiazygos veins.
- hemiazygos vein: the "inferior" (spatially) partner of the azygos vein. It ascends as far as T9 or so, receiving blood from the left posterior intercostal veins and many of the smaller veins draining the mediastinal viscera, before crossing the vertebral column to join the azygos vein.
- accessory hemiazygos vein: the azygos vein's "superior" partner, running along the left side of the spinal column between T5 and T8. It receives those posterior intercostal veins and others, before crossing the vertebral column to join the azygos vein.
- Thoracic duct: drains all of the lymph from all of the body below the diaphragm and the left half of the body above the diaphragm. In the superior mediastinum it can be found behind the aortic arch, on the left side of the esophagus. (W&B 412)
12. Describe the organization of the thoracic sympathetic trunk, in addition to its visceral and splanchnic branches. (W&B 413-416, N158, N160, N165, N209, N240, N254, TG4-45, TG4-46, TG8-03, TG8-14)This set of cross-sections might help (no guarantee!):
The thoracic sympathetic trunk is the inferior continuation of the cervical sympathetic trunk, and after piercing the diaphragm, continues as the lumbar sympathetic trunk. The trunk is really just a highway for preganglionic sympathetic nerves (thoracolumbar) that need to reach levels superior or inferior to their level of origin in the spinal cord. The chain ganglia along the trunk are the sites of synapse between preganglionic neurons and postganglionic fibers (see box below).
A preganglionic (presynaptic) sympathetic neuron originates in the lateral horn of the spinal cord gray matter. It leaves the cord via the spinal nerve and enters the trunk via a white ramus communicans. The neuron can: a) immediately synapse in the ganglion, or b) travel up or down the trunk, subsequently synapsing in a ganglion superior or inferior to the level of origination of the neuron. In either case, the postganglionic (postsynaptic) neuron then leaves the ganglion via the gray ramus communicans to rejoin the spinal nerve for the purpose of distribution to its target, either via the ventral primary ramus or the dorsal primary ramus.
Besides the three paths mentioned above (up or down via the trunk, or out via the corresponding spinal nerve) there are two other paths that a sympathetic fiber can take. First, some enter visceral branches that directly innervate the smooth muscle, cardiac muscle, and glands of the thoracic viscera. There are contributions to the cardiac, pulmonary, esophageal, and aortic plexuses. Also, there are thoracic splanchnic nerves (Greek, splanchna = viscera), which are preganglionic fibers that travel into and synapse within the abdomen to provide sympathetic innervation for most of the abdominal viscera. (This can be a confusing point. The thoracic splanchnic nerves innervate abdominal viscera. Also, the label "splanchnic" refers to the innervation of viscera, not to a specific origin or make-up. You will see lumbar, pelvic, and sacral splanchnics that are not necessarily pre-ganglionic sympathetic nerves from the sympathetic chain.) These are listed here:
Nerve Level of Origin Site of Synapse greater thoracic splanchnic n. T5 - T9 celiac ganglion, superior mesenteric ganglion, suprarenal medulla lesser thoracic splanchnic n. T10 - T11 aorticorenal ganglion least thoracic splanchnic n. T12 renal plexus
Autonomic Nervous System
The autonomic nervous system, made of the parasympathetic nervous system and the sympathetic nervous system, controls all of the smooth muscle in our body, as well as performing some other specialized functions that will be presented in physiology. Smooth muscle is present throughout the body, in blood vessels and skin, but is most often considered in the context of thoracic, abdominal, and pelvic viscera.
In that it innervates muscle, causing contraction or relaxation, the ANS is similar to the system of skeletal muscle innervation. However, the structures of the two systems is different, hence the necessity to learn words like "synapse", and "ganglion". The nerves to skeletal muscle leave the CNS, travel to the muscle, and do their business at the neuromuscular junction. Sympathetic and parasympathetic nerves, however, take a detour along the way. In the ANS, there are two separate neurons that separate the spinal cord from the target, the preganglionic (presynaptic) and the postganglionic (postsynaptic) neurons. What do you suppose is in the middle of the two? Yep, a ganglion. What happens in a ganglion? A synapse.
Preganglionic sympathetic neurons will leave the spinal cord (in the thoracic and lumbar regions) and travel part-way to their target, either via the sympathetic trunk or a splanchnic nerve. Within that trunk or at the end of that splanchnic nerve, there is a ganglion within which the preganglionic sympathetic neuron will synapse with the postganglionic sympathetic neuron. The postganglionic sympathetic neuron will then travel to the target, usually smooth muscle of an arteriole, but also cardiac muscle, sweat glands, and errector pili muscles (small muscles in the skin that attach to hair follicles and can give you "goose bumps").
Preganglionic parasympathetic neurons usually leave the spinal cord (in the cranial and sacral regions) and travel directly to their target organ, sometimes piggybacking on splanchnic or other nerves. They will synapse in very small ganglia in or on the target organ. The postganglionic parasympathetic neurons, then, do not travel very far to reach their target tissue (usually smooth muscle or glands, but also cardiac muscle).
One more thing: You will come across abbreviations, either in the anatomy tables or some texts, like GVE, SVA, GSE, etc. This is old terminology that divided innervation up into general vs. special, visceral vs. somatic, and efferent vs. afferent. The current way of thinking, and the way that this course will be taught, divides innervation up functionally, as described above, with skeletal, sympathetic, and parasympathetic nerves, some of which are efferent and some of which are afferent.
Cultural enrichment: Check out these sections from the 1918 version of Gray's Anatomy of the Human Body! Some of the terms are (of course) out-of-date, but the illustrations are timeless.The Trachea and Bronchi - The Lungs - The Pulmonary Veins - The Thoracic Duct - The Vagus Nerve - Surface Anatomy of the Thorax - Surface Markings of the Thorax
Questions and Answers:
1. Are there plexuses of nerves on the pulmonary arteries? (N209, TG4-45, TG8-14, TG8-15)2. Determine the relation of the left superior intercostal vein to the aortic arch, the phrenic nerve, and vagus nerves. (N231, TG4-36B)The pulmonary plexuses lie around the roots of the lungs, and the pulmonary artery is one of the structures of the lung roots. Therefore, there are plexuses on the arteries.
3. Observe the formation of the superior vena cava (confluence of both brachiocephalic veins), and relate its position to the manubrium and other great vessels. (N N196, N206, N212, TG4-37B, TG4-15, TG4-19)The left superior intercostal vein runs between the vagus and phrenic nerves. It crosses the aortic arch horizontally passing from the heads of the ribs anteriorly to end in the left brachiocephalic vein.
4. Are there cardiac nerves arising from the left vagus? (N209, N240, TG4-45, TG8-15)The superior vena cava lies immediately to the right of the manubrium. It is overlapped on its left margin by the ascending aorta. Posteriorly, it lies against the right pulmonary artery and the right superior pulmonary vein.
5. Do you find a vertebral artery from the arch of the aorta? (N33)The left vagus normally gives parasympathetic branches to the cardiac plexus. They are most easily seen where the vagus crosses the aortic arch.
6. Pull the aortic arch toward the left and observe the thoracic portion of the trachea. What innervates it and how? (N209, N240, TG4-35, TG4-45)Sometimes the left vertebral artery will branch directly from the aortic arch.
7. What is the blood supply of the trachea? What structure does it lie upon? (N33, N207, TG7-14, Objective 4)The recurrent laryngeal nerves innervate the upper trachea and esophagus as they pass superiorly in the tracheoesophageal groove to reach the larynx, which they also innervate. Recurrent laryngeal nerves provide skeletal motor innervation to the voluntary muscle of upper esophagus and larynx and parasympathetic motor innervation to the smooth muscle of the trachea. They also provide parasympathetic motor innervation to the mucous glands of all of these structures.
8. Locate the right and left bronchial arteries. What is their source? How do the two sides differ in number? (N207, TG4-39)For the blood supply, see Objective #4 above. The trachea lies upon the esophagus.
9. What is the difference between the "root" of the lung and the "hilum"? (N199, TG4-31AB, TG4-31CD)The two left bronchial arteries are branches from the highest part of descending aorta. The single right bronchial artery is either a branch of one of the left bronchial arteries or it may branch from the right 3rd posterior intercostal artery, in which case the common trunk is called the intercostobronchial trunk.
10. How do the cardiac and pulmonary plexuses differ? Where do they distribute? (N209, N240, TG4-45)The root of the lung is the collection of structures that connect the lung to the mediastinum. This includes the pulmonary arteries and veins, the primary bronchi and bronchial arteries, and the pulmonary nerve plexuses and lymphatics. The hilum is the place on the lung where these structures enter and leave the lung.
11. Where and what is the cardiac notch? (N199, TG4-30AB, TG4-31AB)The cardiac and pulmonary plexuses are continuous at the tracheal bifurcation. The heart receives the cardiac plexus and lungs the pulmonary plexus.
12. What is the average projection of each lung and its fissures to the rib cage? (N196, N 197, N200, TG4-15, TG4-16, TG4-30C)The cardiac notch is a lateral deviation in the anterior border of the left lung, caused by the position of the heart. The lingula is an anterior projection of the left superior lobe below the cardiac notch.
13. What is the lingular bronchus? (N202, N 203, TG4-33A)The anterior borders of each lung generally follow the sternal margin, although the cardiac notch causes a lateral deviation to the left anterior border between the 4th and 6th ribs. The apex of each lung projects to the level of T1, which means, due to the declination of the first rib anteriorly, that the apex rises above the first rib. The inferior border of each lung is located at rib 6 in the midclavicular line, rib 8 at midaxillary line, and rib 10 in the paravertebral line. (Recall that the pleura goes 8, 10, 12.) Both oblique fissures begin posteriorly at the spine of T3, passing obliquely (like the name implies) to reach the 6th costal cartilage near the midclavicular line. The horizontal fissure of the right lung begins at rib 5 in the midaxillary line, then reaches rib 4 to follow it anteriorly to the sternal margin.
14. What is its significance of the superior segmental branch of the right inferior lobar bronchus? (N203, TG4-33A)The left superior lobe bronchus has two divisions: superior and lingular. The lingular division or lingular bronchus has two segmental bronchi: superior lingular and inferior lingular.
15. Are there sympathetic branches to the lung? Along what do they distribute? (N209, N240, TG4-45, TG4-46, TG8-14)Due to its larger caliber and more vertical orientation, the right primary bronchus is more likely to receive foreign bodies that enter the airway. The superior segmental bronchus branches posteriorly off of the intermediate bronchus or the inferior lobe bronchus, so it is the most likely segmental bronchus to receive those foreign bodies that enter the right bronchus. This is especially true if the patient is in a supine position.
16. Where does the esophagus begin? Where does it pass into the abdomen? Where does it terminate? (N63, N194, N195, N232, N234, N235, TG4-45, TG4-46)Sympathetic fibers reach the lungs via the pulmonary plexuses, which are located along the roots of the lungs. Pulmonary plexuses are continuous with the cardiac plexus at the tracheal bifurcation. Additional sympathetics reach the pulmonary plexuses via the thoracic visceral nerves, which are branches from T1-T4/T5 sympathetic chain ganglia.
17. Consider the course, relations, constrictions of the esophagus. (N232, TG4-49, TG7-91)The laryngopharynx "becomes" the esophagus at the C6 level. The esophagus passes through the esophageal hiatus of the diaphragm, which is at the T10 level, to end in the cardiac portion of the stomach.
For course and relations, see above. Constrictions of the esophagus are found at its beginning, at the tracheal bifurcation, and at the esophageal hiatus.18. Describe the blood supply and venous drainage of the esophagus. Are there venous collaterals to stomach? (N238, TG4-49, TG7-91)19. Do the right and left mediastinal pleurae come together? (N194, TG4-49)Two or three esophageal arteries branch from the descending aorta. Esophageal veins drain into the azygos system, which eventually reaches the superior vena cava. The esophageal tributaries of the left gastric vein drain the terminal esophagus. Since the gastric veins first drain into the portal system before going to the heart, this part of the esophagus is an important site of portal-caval (portal-systemic) anastomosis in cases of portal hypertension.
20. Through what and at what level does the aorta enter the abdominal cavity? (N194, N195, TG4-37, TG4-38, TG4-39)Very low in the posterior mediastinum the esophagus sweeps forward, so there is potential for the right and left mediastinal parietal pleurae to touch one another posterior to esophagus and anterior to aorta. However, typically the anterior deviation of the esophagus is not sufficient to allow enough space for this contact of the pleurae.
21. What is the subcostal artery? (N264, TG4-49, TG7-91, TG4-39)The descending thoracic aorta passes through the diaphragm at the aortic hiatus, a passageway between the two diaphragmatic crura, located at the T12 level.
22. Completely review the blood supply to an intercostal space. (N33, N191, N192, TG4-43)Below the 12th rib, there is no intercostal space or intercostal artery, so we call the segmental neurovascular structures subcostal.
23. What are the posterior branches of the posterior intercostal (segmental) arteries? What do they supply? (N171, N172, TG4-39, TG4-08)Intercostal spaces in general are supplied by posterior and anterior intercostal arteries. Posterior intercostal arteries 3 through 11 are branches of the descending thoracic aorta. The first two posterior intercostal arteries are branches of the highest intercostal artery, which is a branch of the costocervical trunk from subclavian artery. Anterior intercostals are branches of the internal thoracic or the musculophrenic arteries.
24. Observe the azygos venous system. If you have two primary veins, do they communicate with one another? How? Where? What is the pattern of venous drainage in your specimen? Are all the veins present? If not, where does the drainage go? (N238, TG4-38, TG4-39, TG4-40)The posterior branches of posterior intercostal arteries supply the deep and superficial back muscles, skin of the back, and the vertebral column. They have radicular branches that reach the spinal cord along the dorsal and ventral rootlets.
25. What vein drains the first intercostal space? Into what? What veins drain into the azygos system? (N238, TG4-38, TG4-39, TG4-40)Hemiazygos and accessory hemiazygos usually cross the midline at T7, 8, or 9 to empty into the azygos vein. There are also connections between the various left-sided venous channels.
26. How does the thoracic duct get into the thorax? At what level does it deviate to the left side? (N206, N266, TG4-43, TG4-44)Both first posterior intercostal veins drain directly into their respective brachiocephalic veins. Bronchial and esophageal veins drain into the azygos system, the latter being a significant site of portal-caval anastomosis in cases of portal hypertension. (This is the second mention... could be important!)
27. Do you find posterior mediastinal lymph nodes or afferent lymph channels? (N239, TG4-43, TG4-44)The thoracic duct enters the chest through the aortic hiatus along the right side of the aorta. It deviates to the left at the level of the sternal angle. (The trachea pushes the esophagus against the vertebral bodies which pushes thoracic duct to the left.)
28. What are bronchomediastinal lymph trunks? (N208, TG4-43, TG4-44)The thoracic duct is usually paralleled by posterior mediastinal nodes.
29. Is the sympathetic trunk located within the posterior mediastinum? Does it change positions in different regions of the chest? (N N180, N254, TG4-45, TG4-46, TG8-14)The lymph from the lungs and chest passes through the paratracheal nodes to form the bronchomediastinal lymph trunks. These drain to the thoracic duct on the left and the right lymphatic duct on the right.
30. How many thoracic ganglia do you find? (N209, N240, TG4-45, TG4-46, TG8-14)The sympathetic trunk lies on the heads of the ribs through most of the chest, so it is almost, but not quite, within the posterior mediastinum. It deviates anteromedially as it travels inferiorly to its exit through the diaphragm.
31. Identify white and gray rami communicans. What is their significance and distribution? What do they contain? (N164, N180, N209, N240, N254, TG4-45, TG4-46, TG8-14)There are typically 12 thoracic ganglia, although the first may be fused with the inferior cervical ganglion to form a cervicothoracic (stellate) ganglion.
32. Do you see thoracic visceral nerves to the aorta, esophagus, and trachea? What about to the cardiac and pulmonary plexuses? (N209, N240, TG4-45, TG4-46, TG8-03, TG8-14)Since the preganglionic sympathetic neurons live within the spinal cord at T1 to L2 levels, these are the only levels where white rami communicans are found. Gray rami, on the other hand, are found at every level at which there are spinal nerves. Gray rami carry postganglionic sympathetic fibers back to the ventral primary rami, to be distributed along their branches (and also the branches of the dorsal primary rami).
33. Expose the greater (thoracic) splanchnic nerve. From what does it come? At what level? What types of fibers does it contain? To what does it distribute? (N209, TG4-45, TG4-46, TG8-03, TG8-14)The first 4 or 5 thoracic ganglia (T1-4) give small visceral branches that pass anteroinferiorly to reach the cardiac, pulmonary, esophageal, and aortic plexuses, as well as the trachea.
The greater thoracic splanchnic nerve is made by contributions from sympathetic chain ganglia at T5 to T9 (or T10) levels. These are preganglionic fibers that leave the chest to enter the abdomen. They synapse in the celiac ganglion and innervate the abdominal viscera that is supplied by the celiac trunk.