
|
|
|
||||||||||||
Dissector Answers - Hand |
|||||||||||||
Learning Objectives:
Upon completion of this session, the student will be able to:
- Describe the position of tendons, associated bursae, nerves, and vessels beneath the palmar carpal ligament.
- Identify the prominent features of carpals, metacarpals and phalanges associated with the hand as listed in the lab manual.
- Define the thenar, hypothenar, central, and adductor-interosseous compartments of the hand and the functional significance of each.
- Correlate any fractures or deep cuts of the hand with functional disruptions of associated muscular and neurovascular structures.
- Describe the movements of the fingers and thumb.
- Describe the collateral circulation of the hand.
Learning Objectives and Explanations:
1. Describe the position of tendons, associated bursae, nerves, and vessels beneath the palmar carpal ligament.This needs about 1,000 words. (W&B 149, N461, N462, TG2-24, TG2-34A, TG2-34B)
2. Identify the prominent features of carpals, metacarpals and phalanges associated with the hand as listed in the lab manual. (W&B 154-156, N452, N456, TG2-31, TG2-32)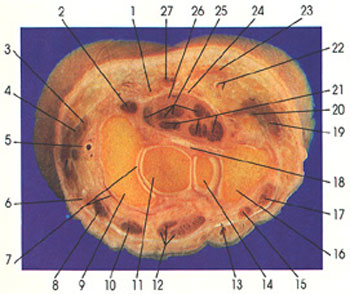
left upper quadrant left lower quadrant right lower quadrant right upper quadrant
- Palmar carpal ligament
- Tendon of flexor carpi radialis m.
- Tendon of extensor pollicis brevis m.
- Tendon of abductor pollicis longus m.
- Radial a.
- Tendon of extensor carpi radialis longus m.
- Articular cavities
- Tendon of extensor carpi radialis brevis m.
- Scaphoid
- Tendon of extensor indicis m.
- Capitate
- Tendon of extensor digitorum communis m.
- Extensor retinaculum
- Hamate
- Tendon of extensor digiti minimi m.
- Triquetral
- Tendon of extensor carpi ulnaris m.
- Radiate carpal ligament
- Abductor digiti minimi m.
- Tendon of flexor carpi ulnaris m.
- Tendons of flexor digitorum profundus m.
- Ulnar a. and n.
- Palmaris brevis m.
- Flexor retinaculum
- Tendons of flexor pollicis longus and flexor digitorum superficialis mm.
- Median n.
- Tendon of palmaris longus m.
3. Define the thenar, hypothenar, central, and adductor-interosseous compartments of the hand and the functional significance of each. (W&B 158-169, N447, N448, N459, N460, N461, N465, N466, N468, N472A, N472B, N476, N477, N479, TG2-34A, TG2-34B, TG2-35A, TG2-35BC)
- carpals: These eight small bones of the wrist are held together by ligaments and arranged in two (irregular) rows, proximal and distal. The bones of the proximal row, listed from the radial to the ulnar side, are the scaphoid, the lunate, the triquetrum, and the pisiform. In the distal row, from radial to ulnar side, are the trapezium, the trapezoid, the capitate, and the hamate. Read across the proximal layer of bones: Send Louis To Paris. Read across the distal layer of bones: To Tame Carnal Hunger, or the more racey: Some Lovers Try Positions That They Can't Handle. Can you guess which is the favorite of medical students? (Note that the pisiform bone is a sesamoid bone in the tendon of the flexor carpi ulnaris, so it sits on the volar surface of the triquetrum.)
- metacarpals: There are five metacarpal bones, numbered from 1 (the thumb) to 5 (the little finger). These bones are just distal to the carpals.
- phalanges: There are fourteen of these "bones of the fingers." The thumb has only two phalanges, a proximal and distal, whereas the other digits each have three phalanges, proximal, middle, and distal.
4. Correlate any fractures or deep cuts of the hand with functional disruptions of associated muscular and neurovascular structures.The hand is entirely wrapped in fascia, with the palmar and dorsal fascia being continuous with one another on both sides. This fascia is relatively thin, except in a triangular area on the middle of the palm. Here the fascia, which is also connected to the flexor retinaculum and palmaris longus tendon (if present) is called the palmar aponeurosis. Furthermore, just like in the lower limb and in the arm and forearm, there are septa that further divide the space into compartments.
In the palm of the hand, there are three important septa. The lateral fibrous septum runs from the lateral part of the palmar aponeurosis to the deep aspect of the third metacarpal. This septum is the border between the thenar compartment lateral to it (towards the thumb) and the central compartment medial to it. Similarly, the medial fibrous septum runs from the medial aspect of the palmar aponeurosis to the deep part of the fifth metacarpal. It separates the hypothenar compartment, which is medial, towards the little finger, from the aforementioned central compartment. Finally, a septum runs medially from the medial side of the first metacarpal to the deep part of the third metacarpal. It separates the more superficial thenar compartment from the deeper adductor compartment.
The intrinsic muscles of the hand are listed below, divided by compartment.
thenar compartment:
adductor/interosseous compartment:
hypothenar compartment:
central compartment:
And finally, we have poor little palmaris brevis muscle. As if it isn't bad enough that the palmaris longus muscle is highly variable, its little brother, the palmaris brevis muscle, is thin, largely insignificant mechanically, and is superficial to, not in, the hypothenar compartment. It does serve to protect the ulnar nerve and artery, which it does valiantly, as well as give you that funny little skin pucker when you make a tight fist.
Muscle Origin Insertion Action Innervation Blood Supply palmaris brevis fascia overlying the hypothenar eminence skin of the palm near the ulnar border of the hand draws the skin of the ulnar side of the hand toward the center of the palm superficial br. of the ulnar n. ulnar a. To summarize innervation, there are two main nerves. The median nerve gets the thenar muscles via its recurrent (motor) branch, as well as half of the lumbricals. The deep branch of the ulnar nerve gets all of the rest, with the exception of the palmaris brevis muscle, which is innervated by a superficial branch of the ulnar nerve.
5. Describe the movements of the fingers and thumb. (W&B 13-14, N463, N464, N465, TG2-45, TG2-24)The two classic examples here both involve the median nerve:
Injury to the median nerve at the wrist, in, say, a case of carpal tunnel syndrome, results in severe paralysis of some hand motions and loss of cutaneous sensation. Most noticeable is the loss of the ability to oppose the thumb, since the only muscle that does this for the thumb is an intrinsic hand muscle innervated by the median nerve, the opponens pollicis muscle. (Other intrinsic muscles of the hand can call for back-up from forearm muscles, to, for example, flex the thumb or little finger. These actions will, of course, be weakened somewhat.) (Hint: Know about carpal tunnel syndrome.)
Often, farm equipment, switchblades, or broken glass can produce a direct wound to the thenar eminence, possibly injuring the recurrent (motor) branch of the median nerve itself. This also paralyzes the muscles of the thenar eminence, and causes subsequent wasting of the area. But, depending on what branches had already been given off, the lesion may be less severe than one caused farther up the chain at the wrist.
Other injuries are of course possible. Use your imagination to figure out what things one could cut when falling with arms outstretched through a plate-glass window, then use the tables to figure out how that person would present to you in the Emergency Department.
6. Describe the collateral circulation of the hand. (W&B 185, N466, N469, TG2-37A, TG2-37B)The flexion and extension of the fingers is pretty straightforward. Abduction and adduction of them is the same as with the toes, with the third digit (2nd finger, "middle" finger) held as the axial line. The other three fingers either move toward (adduction) or away from (abduction) this finger.
The thumb gets to be a little tricky. Opposition is where you bring the pad of the thumb into contact with the pad of another digit, often specifically the little finger. This "simple" motion, which sets us apart from all but our closest monkey cousins, is really quite complex. But, the rest of the "standard" motions of the thumb are defined differently than for the other digits. Abduction is bringing the thumb out, away from the plane of the palm. Make a hand puppet, then straighten your MP joints. Your thumb is abducted. Clearly, bringing it back, then, is adduction. Extension of the thumb takes place as you move it away from the other digits within the plane of the palm, like when hitchhiking or making the "L for loser" sign on your forehead. Flexion is not only bringing it back, but then further moving it such that it is lying across the palm.
There are a bunch of places in the hand where arterial anastomosis occurs:
- both the superficial and deep palmar arches get blood from both the radial and ulnar arteries
- palmar metacarpal arteries with the common palmar digital arteries
- the perforating branches of the dorsal metacarpals with both the deep palmar arch and the common palmar digital arteries
- the proper dorsal arteries with the palmar digital arteries
Cultural enrichment: Check out these sections from the 1918 version of Gray's Anatomy of the Human Body! Some of the terms are (of course) out-of-date, but the illustrations are timeless. The Anterior Divisions (nerves) - The Veins of the Upper Extremity and Thorax - The Brachial Artery - The Radial Artery - The Ulnar Artery - The Muscles and Fascia of the Forearm - The Muscles and Fascia of the Hand - Surface Anatomy of the Upper Extremity - Surface Markings of the Upper Extremity
Questions and Answers:
7. Locate the palmar digital branches of the median and ulnar nerves along the borders of the digits. Determine area of distribution. Do they supply any portion of the dorsal side of the digit? How much? Significance? What do they accompany?The proper palmar digital branches of median nerve reach the radial 3 and 1/2 digits, while the ulnar branches reach the remaining ulnar 1 and 1/2 digits. Each palmar digital branch sends branches onto the dorsal surface of the distal phalanx, to supply the nail bed. Proper palmar digital arteries, primarily from the superficial palmar arterial arch, travel with the nerves. (N468,N472A, TG2-33B, TG2-38A)8. What is the relation of the palmar aponeurosis to palmaris longus tendon, the palmar carpal ligament, and the flexor retinaculum?The palmaris longus tendon spreads to unite with the palmar aponeurosis. The tendon passes deep to the palmar carpal ligament, and superficial to the flexor retinaculum. (N459, N460, N461, TG2-23, TG2-24)9. Identify the superficial transverse metacarpal ligament and transverse fasciculi and note the gaps between them. What can be seen in these gaps?The common palmar digital neurovascular bundles can be found dividing into their proper palmar digital branches in these gaps. (N459, TG2-33)9a. What is the carpal tunnel and its associated syndrome?The anatomy tables cover it well. It says that carpal tunnel syndrome: "results from any lesion that significally reduces the size of the carpal tunnel. Fluid retention, infection, and excessive exercise of the fingers may cause swelling of the tendons or their synovial sheaths. Median nerve is the most sensitive structure in the carpal tunnel and therefore is the most affected. Median nerve has sensory branches to the lateral three and a half digits thus paresthesia (abnormal sensation), hypothesia (reduced sensation), or anesthesia (loss of sensation) may occur. Furthermore, the main motor branch of the median nerve is the recurrent branch which serves three thenar muscles (it also serves the radial 2 lumbricals via common palmar digitals). Continued compresion of the median nerve will lead to weakness of the abductor pollicis brevis and opponens pollicis. To relieve the symptoms, partial or complete surgical division of the flexor retinaculum (carpal tunnel release) may be necessary. Clinically this syndrome can be tested for by tapping on the carpal tunnel. If symptoms are elicited (positive Tinel's sign), the syndrome is likely." (N461,N472A,N475, TG2-34A, TG2-34B, TG2-35)10. What artery completes the superficial palmar arterial arch?The superficial palmar branch of the radial artery completes the superficial palmar arterial arch. (N466, TG2-37)10a. How do median and ulnar nerves share in the cutaneous innervation of the digits (review)?Median nerve branches reach the radial 3 1/2 digits, while ulnar branches reach the remaining ulnar 1 1/2 digits. This includes the dorsal surface of the distal phalanx, to supply the nail bed. (N472, TG2-33, TG2-38)11. Does the flexor pollicis brevis muscle have a deep head?Yes, the deep head arises from the trapezoid and capitate, while the superficial head arises from the flexor retinaculum and the trapezium. (N465, TG2-34)12. Trace the superficial palmar branch of the radial artery to the thenar compartment. Does it continue beyond the compartment? Where?The superficial palmar branch of radial artery completes the superficial palmar arch by passing into the central compartment, deep to the palmar aponeurosis. (N466, TG2-37A, TG2-37B)13. What is the source of innervation for the hypothenar muscles?As discussed in #3 above, the deep branch of ulnar nerve innervates these muscles. It passes between the abductor digiti minimi and flexor digiti minimi brevis muscles. (N465,N476, TG2-34A, TG2-34B)14. Examine the contents of the carpal tunnel. How is it formed?The carpal tunnel is formed by the attachment of the flexor retinaculum to the trapezium and scaphoid laterally, and the hook of the hamate and the pisiform medially. (N461, TG2-34)15. Into which digital sheath does the ulnar bursa continue distally?The ulnar bursa continues into the sheath for the little finger flexor tendons, which means that an infection of the little finger involving its flexor and synovial sheaths could lead to an infection within the carpal tunnel. (N464, TG2-34)16. What are vincula?Vincula (mesotendons) are folds of synovial membrane containing neurovascular pedicles supplying the flexor tendons. They are located between the phalanges and the flexor tendons. (N464, TG2-45)17. Identify the lumbrical muscles, noting origin. Trace them to their immediate and functional insertion. What is the course of innervation?The radial 2 lumbricals are innervated by the median nerve, via its palmar digital branches. The ulnar 2 lumbricals are innervated by the ulnar nerve. (N463, N464,N475,N476, TG2-34A, TG2-34B)18. Locate the flexor carpi radialis tendon. Is it in the carpal tunnel? What happens to it?The tendon of flexor carpi radialis traverses a split in the flexor retinaculum to insert on the bases of the second and third metacarpals. (N461, TG2-36)19. Consider the complete blood supply to the hand, including sources and arches . How do the dorsal and palmar proper digital arteries differ in their formation? What are perforating arteries? Where are they found? What is their function?The superficial palmar arch is formed by the superficial branch of the ulnar artery and the superficial palmar branch of the radial artery. The deep palmar arch is primarily formed by the radial artery anastomosing with the deep branch of the ulnar artery. Dorsal carpal branches of radial and ulnar unite to form a dorsal carpal arch. This arch gives off dorsal metacarpal arteries which divide into the dorsal digital arteries. Palmar digital arteries are branches of common digital branches of the superficial arch. Perforating arteries connect the dorsal and palmar metacarpal arteries (from the deep arch) at the heads of the metacarpal bones. (N466, TG2-37A, TG2-37B)