|
|
|
||||||||||||
Dissector Answers - Kidneys & Retroperitoneum |
|||||||||||||
Learning Objectives:
Upon completion of this session, the student will be able to:
- Demonstrate the relationships of the kidneys and suprarenal glands to adipose and fascial coverings, lower ribs and other abdominal organs.
- Describe the basic internal gross anatomy of the kidney.
- Define the blood supply and drainage of the kidneys and suprarenal glands.
- Describe the general organization of the urinary and endocrine systems.
- Know the pattern of diaphragmatic musculature and its fasciae, and its functional significance in respiration.
- Know the three major passageways through the diaphragm and the structures traversing them.
- Describe the position and vertebral level for all branches of the abdominal aorta and the inferior vena cava, and the reason for the difference in their patterns.
- Identify the thoracic and lumbar splanchnic nerves and the collateral ganglia or regional subdivisions of the preaortic plexus to which each functionally relates.
- Recall the concept of perivascular plexuses, their position, nomenclature, and nerve fiber components.
- Describe the parasympathetic innervation of the GI tract.
- Identify the cisterna chyli and describe the general pattern of lymphatic drainage to the thoracic duct.
- Identify and demonstrate the abdominal attachments of the two major posterior abdominal wall muscles and know the action of these muscles upon the vertebral column.
- Describe the nerves of the lumbar plexus in terms of their: spatial relationship to the posterior abdominal wall muscles; distribution to the abdominal wall, the genital region, and the lower limb; and categorization into purely cutaneous nerves and those which also innervate muscles.
- Locate the lumbar sympathetic trunk and white and gray rami communicantes; explain the reason for the inferior limit of the white rami.
Learning Objectives and Explanations:
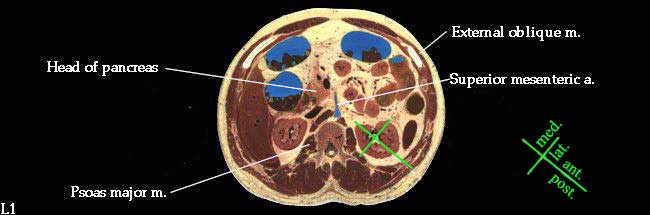
1. Demonstrate the relationships of the kidneys and suprarenal glands to adipose and fascial coverings, lower ribs and other abdominal organs. (W&B 489-493, N 273,329,330,354 or TG 5-30, 5-31, 5-42)2. Describe the basic internal gross anatomy of the kidney. (W&B 491-493, N 334A, 334B or TG 5-32A, 5-32B).The orientation of the kidneys is best illustrated with a cross-section.
Since they lie against the psoas muscle (which lies against the vertebral column), their posterior surfaces are somewhat medial as well, while their anterior surfaces are also lateral. The convex lateral border (the outside of the "bean") is also posterior, and the medial border, with the hilum, is also anterior.
The kidneys are retroperitoneal. Unlike other GI organs that begin development with a mesentery then fuse to the body wall, the kidneys are stuck there from the beginning. Besides their peritoneal covering, each is embedded in two layers of fat, with a membrane, the renal fascia, in between the layers. Inside the renal fascia is the perirenal fat, while outside the membrane is the pararenal fat. (The perirenal layer is inside, while the pararenal layer is around the renal fascia.)
With regard to the relationships of the kidneys to other structures, we can think about the posterior and the anterior surfaces. The superior 1/3 of the posterior surface lies against the diaphragm. The remaining 2/3 is inferior to the diaphragm, and therefore contacts the quadratus lumborum muscle. The subcostal nerve and vessels run posterior to the kidneys on either side. (The kidney is somewhat protected by the twelfth rib.)
The anterior relationships are different on each side, except that both kidneys are capped superomedially by a suprarenal (adrenal) gland. The right kidney contacts the descending (2nd) portion of the duodenum, the right lobe of the liver, the right colic (hepatic) flexure, and some coils of jejunum. The left kidney contacts the pancreas, the stomach, the spleen, the left colic (splenic) flexure, and some coils of jejunum.
3. Define the blood supply and drainage of the kidneys and suprarenal glands. (N 332,335 or TG 5-31, 5-32)The kidney is one of several organs in the body that has some sort of cortex (Latin, cortex = bark) around the outside, surrounding an inner medulla. The renal medulla is divided into renal (medullary) pyramids, with renal columns, made of cortical tissue, between them. The renal pyramids have their apex, or renal papilla, pointed toward the center of the kidney. Here the tubules dump into first minor calicies, which then join with others to form major calicies, and finally the renal pelvis. The renal pelvis is the proximal, dilated portion of the ureter.
4. Describe the general organization of the urinary and endocrine systems. (W&B 493, N 341 or TG5-30)Both kidneys are supplied by renal arteries, both of which branch directly from the abdominal aorta slightly inferior to the branching point of the SMA. The renal arteries travel to each kidney, each one posterior to its respective renal vein, which drain directly into the IVC. (Because the aorta runs slightly to the left of midline, and the IVC is significantly right of midline, the arteries and veins have different lengths. The right artery is a little longer than the left, passing behind the IVC and the point of junction of the right renal vein and the IVC. The right vein is very short. On the left side, the left artery, which is a bit shorter than the right, emerges from the aorta and runs posterior to the left vein. The left vein has a very long trip back over to the right side and the IVC.) On both sides the arteries branch multiple times, into segmental arteries, before entering the hilum of the kidney both anterior and posterior to the renal pelvis. The veins follow a similar pattern, with multiple tributaries coming out of the hilum of the kidney to coalesce to form the renal vein. As far as circulation within the kidney goes, know that the segmental arteries run in the renal columns, and that there are no anastomoses between them. (See W&B 492-493 or a histology text for the somewhat complicated pattern of vessels that branch from there.)
The suprarenal (adrenal) glands are extremely vascular. (According to W&B, relative to size, more blood flows through them than any other organ, with the possible exception of the thyroid gland.) They receive blood from three sources, all of which branch into varying numbers of twigs before entering the gland.
- superior suprarenal arteries: from the posterior branches (usually) of the inferior phrenic arteries
- middle suprarenal arteries: one or more branches on each side from the abdominal aorta
- inferior suprarenal arteries: from the respective renal arteries
Most of the venous drainage, which is important since it carries all of the goodies made by the gland, is via the suprarenal (central suprarenal) veins. The left one drains into the left renal vein while the right one drains directly into the IVC.
Note: The renal arterial supply is extremely variable. In fact, the "Illustrated Encyclopedia of Human Anatomic Variation" suggests that "it is not only ludicrous but dangerous to suggest that the kidneys each receive only a single artery."
For more than you ever wanted to know about anatomical variation, the University of Iowa has a great site, an "Illustrated Encyclopedia of Human Anatomic Variation". Here is a quick and dirty link to the section on renal arteries.
5. Know the pattern of diaphragmatic musculature and its fasciae, and its functional significance in respiration. (W&B 497-499, N 194,195,263 or TG5-33)The urinary system consists of the kidneys, ureters, urinary bladder, and urethra. The kidneys filter the blood, then collect and concentrate the waste products. This waste water travels in the ureters from the kidney to the urinary bladder, where it is stored until it is excreted at a convenient time. The bladder pushes its contents out of the body via the urethra. In females it is a short trip to the outside of the body, while in males, the urethra must travel through the penis. (Latin, urinari = to dive)
The endocrine system is a collection of ductless glands that are scattered about the body. They make chemical signals, or hormones, in response to internal or external stimuli. These hormones are usually released into the blood, where they traverse the entire circulation to reach their target. The suprarenal (adrenal) glands are very important in that they regulate water/ion balance, various aspects of metabolism, part of sexual development, and the "fight or flight" response.
6. Know the three major passageways through the diaphragm and the structures traversing them. (W&B 499, N 194,195,263 or TG 5-33)
This view of the diaphragm shows all of the structures from which the muscle fibers take origin. The diaphragm is divided into three parts on the basis of these muscle fiber origins:
- sternal part: small origin of muscle on the posterior aspect of the xiphoid process
- costal part: origins from the cartilage and bone of the lower six ribs
- lumbar part: all of the rest, including origins from the bodies of the first three lumbar vertebrae (forming two crurae) and from the arcuate ligaments (labeled "lumbocostal arches" above).
Think of the diaphragm as a round dome tent. All of the fibers originate from the ground, where the tent is staked down. The stakes in front are the xyphoid process, those in back are the lumbar vertebrae. The posterolateral stakes are the arcuate ligaments, while the anterolateral stakes are the ribs. They all insert into the central tendon, which is the top of the tent where everything comes together.
Some parts of the diaphragm are:
- right crus: takes origin from L1-L3. It splits to enclose the esophagus, so the esophageal hiatus is (usually) entirely formed by the right crus. Fibers from the right crus intermingle with the fibers from the left crus at the aortic hiatus. (Latin, crus = resembling leg or legs)
- left crus: takes origin from L1-L2. It is smaller and shorter than the right crus. It sometimes contributes something to the esophageal hiatus. Fibers from the left crus intermingle with the fibers from the right crus at the aortic hiatus. (Latin, crus = resembling leg or legs)
- medial arcuate ligaments: thickening of psoas major fascia. Fibers taking origin from here, along with those from the lateral arcuate ligament, fill in the "gap" between the crura and the costal part of the diaphragm. They are labeled "medial lumbocostal arches" above. (Latin, arcuare = to bend like a bow)
- lateral arcuate ligaments: thickening of the quadratus lumborum fascia. Fibers taking origin from here, along with those from the medial arcuate ligament, fill in the "gap" between the crura and the costal part of the diaphragm. They are labeled "lateral lumbocostal arches" above. (Latin, arcuare = to bend like a bow)
The diaphragm is the primary muscle of respiration. Contraction of the fibers pulls the central tendon inferiorly, increasing the volume (and decreasing the pressure) of the thoracic cavity. Since good ole PV=nRT creates a pressure gradient between the inside and the outside, air rushes in to compensate. Secondary to this, the volume of the abdominal cavity is decreased, raising its pressure. Sometimes you do actually want to do this, like during defecation or parturition. The diaphragm can assist the abdominal wall muscles here.
7. Describe the position and vertebral level for all branches of the abdominal aorta and the inferior vena cava, and the reason for the difference in their patterns. (W&B 507-512, N 264, 265 or TG 5-34, 5-34)
- vena caval foramen: T8 - transmits the IVC, right phrenic nerve branches, and small lymphatic vessels
- esophageal hiatus: T10 - transmits the esophagus, anterior and posterior vagal trunks, branches of left gastric vessels, and small lymphatic vessels (Latin, hiare = to yawn... referring to an interruption)
- aortic hiatus: T12 (not really a hole in the diaphragm, but more of a dent in its edge) - transmits descending aorta, thoracic duct, and sometimes the azygous vein. (Latin, hiare = to yawn... referring to an interruption)
8. Identify the thoracic and lumbar splanchnic nerves and the collateral ganglia or regional subdivisions of the preaortic plexus to which each functionally relates. (W&B 503, N 209,318 or TG 4-38, 5-39)
The tributaries of the inferior vena cava, in part, follow the branches of the abdominal aorta. There are some differences, however. The major one is that the SMV and the IMV are part of the portal system, and therefore have nothing to do with the IVC. Also, the left gonadal veins drain into the left renal vein, instead of directly into the IVC.
9. Recall the concept of perivascular plexuses, their position, nomenclature, and nerve fiber components. (N 318, 319, 322, 323 or TG 5-39,8-16,8-17)The presynaptic (preganglionic) fibers of the thoracic splanchnic nerves originate from the sympathetic trunk in the thorax and run through the diaphragm to provide most of the sympathetic innervation to abdominal viscera. The greater thoracic splanchnic nerve comes from T5-T9 and synapses in the celiac ganglion. The lesser thoracic splanchnic nerve comes from T10-11 and synapses in the aorticorenal ganglion. The least thoracic splanchnic nerve goes from T12 to the renal plexus.
The presynaptic (preganglionic) fibers of the lumbar splanchnic nerves originate from the sympathetic trunk in the abdomen. They provide small fibers to all of the preaortic plexuses, including the celiac, superior mesenteric, intermesenteric, and superior hypogastric plexuses.
The point of all of this is to shut down the GI tract when energy needs to be diverted to other activities. In addition, fibers go to the smooth muscle in the walls of arteries and arterioles to regulate blood flow and blood pressure.
10. Describe the parasympathetic innervation of the GI tract. (W&B 456-457 (stomach), 465-466 (duodenum), 482 (SI), 488 (LI))Perivascular plexuses are just that - plexuses of sympathetic nerves that run along vessels in order to reach their targets. Sometimes they are using the vessel as a convenient roadway to reach a visceral target. In other cases, since blood vessel smooth muscle receives sympathetic innervation, the vessels are the target. They are named according to the vessel upon which they lie.
This is not an enormously important topic, but is one that is worth thinking about. You will see it again, especially while studying the head and neck.
11. Identify the cisterna chyli and describe the general pattern of lymphatic drainage to the thoracic duct. (W&B 412, 501, TG 5-37)We saw the same question in the session on the stomach. Below is the same answer.
Parasympathetic innervation to most of the GI tract, from the stomach to the splenic flexure of the colon, is originally from the vagus nerves (CN X) (N 228,309,310,311,314A,314B or TG 4-37,8-16,8-17). Along the way they will form various plexuses and then reorganize into nerves, but it is all vagus derived. (For example, after the esophageal plexus, fibers come back together to form the anterior and posterior vagal trunks, which supply the stomach and other viscera.) For the portions of the colon distal to the splenic flexure, the parasympathetic innervation is from S2-S4, via the pelvic splanchnic nerves and the inferior hypogastric plexus. (Recall that arterial blood supply to the colon also had a "transition" near the splenic flexure.)
In addition to this information from the previous lab, there is one small point. The parasympathetic fibers coming from the vagus nerve, innervating the GI tract from the stomach through the proximal 2/3 of the transverse colon, follow some of the same paths as the sympathetics from the thoracic splanchnic nerves. So, for example, they will pass through, but not synapse within, the celiac ganglion. Parasympathetic nerves usually synapse within the target tissue.
On the other hand, the parasympathetic fibers that innervate the distal portion of the colon come from S2-S4 via the pelvic splanchnics. They do not follow along the same paths as the sympathetic fibers, which, in this case, go through the inferior mesenteric plexus. Branches of the pelvic splanchnic nerves reach the hindgut by passing up over the left pelvic brim and through the fusion fascia to reach the splenic flexure, and the descending and sigmoid colon. Of course, pelvic splanchnic nerves also distribute to pelvic viscera, such as the rectum, but we can save that story for the pelvis.
12. Identify and demonstrate the abdominal attachments of the two major posterior abdominal wall muscles and know the action of these muscles upon the vertebral column. (W&B 513-515, N 263 or TG 5-33)In 25-50% of cases, the inferior portion of the thoracic duct includes a dilated portion called the cisterna chyli (chyle cistern). When present, all of the lymph trunks draining the abdomen and lower limbs dump into it, as well as the most inferior intercostal lymph trunks. When it is not present, these trunks simply empty into the thoracic duct.
See the pages indicated above for good diagrams of the general pattern of lymphatic drainage of the body. Especially important in the abdomen is the intestinal lymph trunk, which carries all of the fat from those double cheeseburger combo meals from the small intestine to the thoracic duct.
For more than you ever wanted to know about anatomical variation, the University of Iowa has a great site, an "Illustrated Encyclopedia of Human Anatomic Variation". Here is a quick and dirty link to the section on the thoracic duct and cisterna chyli.
The anatomy tables pretty much say it all:13. Describe the nerves of the lumbar plexus in terms of their: spatial relationship to the posterior abdominal wall muscles; distribution to the abdominal wall, the genital region, and the lower limb; and categorization into purely cutaneous nerves and those which also innervate muscles. (W&B 515-517, TG 5-38)
Muscle Origin Insertion Action Notes iliacus iliac fossa and iliac crest; ala of sacrum lesser trochanter of the femur flexes the thigh; if the thigh is fixed it flexes the pelvis on the thigh inserts in company with the psoas major m. via the iliopsoas tendon iliopsoas iliac fossa; bodies and transverse processes of lumbar vertebrae lesser trochanter of the femur flexes the thigh; flexes and laterally bends the lumbar vertebral column a combination of the iliacus and psoas major mm. psoas major bodies and transverse processes of lumbar vertebrae lesser trochanter of femur (with iliacus) via iliopsoas tendon flexes the thigh; flexes & laterally bends the lumbar vertebral column the genitofemoral nerve pierces the anterior surface of the psoas major m. psoas minor bodies of the T12 & L1 vertebrae iliopubic eminence at the line of junction of the ilium and the superior pubic ramus flexes & laterally bends the lumbar vertebral column absent in 40% of cases quadratus lumborum posterior part of the iliac crest and the iliolumbar ligament transverse processes of lumbar vertebrae 1-4 and the 12th rib laterally bends the trunk, fixes the 12th rib the lateral arcuate ligament of the diaphragm crosses the anterior surface of the quadratus lumborum m. 14. Locate the lumbar sympathetic trunk and white and gray rami communicantes; explain the reason for the inferior limit of the white rami. (W&B 503, N N160,N267 or TG 5-38,5-39,5-40,5-41)
Images from "Anatomy of the Human Body" by Henry Gray are provided by:
The description of the formation of the lumbar plexus on W&B 515 is very helpful.
iliohypogastric nerve: from L1 (sometimes with T12 contribution). It runs under the psoas major muscle, emerging at the muscle's lateral border to run over the quadratus lumborum muscle. The iliohypogastric nerve provides motor innervation to the muscles of the lower abdominal wall and sensory innervation to the skin of the lower abdominal wall, upper hip and upper thigh.
ilioinguinal nerve: from L1. It runs under the psoas major muscle, emerging at the muscle's lateral border to run over the quadratus lumborum muscle, inferior to the iliohypogastric nerve. The ilioinguinal nerve provides motor innervation to the muscles of the lower abdominal wall and sensory innervation to the skin of the lower abdominal wall and the anterior labium majus OR scrotum. In a significant number of cases the ilioinguinal is combined with the genitofemoral nerve.
genitofemoral nerve: from L1 and L2. It pierces the psoas major muscle at about the level of L3 or L4. The genitofemoral nerve provides motor innervation to the cremaster muscle (via its genital branch) and sensory innervation to the skin of the anterior labium majus OR scrotum (via its genital branch) and the upper medial thigh (via its femoral branch).
lateral femoral cutaneous nerve: from L2 and L3. It runs under the psoas major muscle, emerging at the muscle's lateral border to run over the iliacus. The lateral femoral cutaneous nerve provides sensory innervation to the skin of the lateral thigh.
obturator nerve: from L2, L3, and L4. It runs along the medial border of the psoas major muscle. The obturator nerve provides motor innervation to the muscles of the medial thigh: the adductor longus m., adductor brevis m., adductor magnus m., gracilis m., and obturator externus m. It provides sensory innervation to the skin of the lower medial thigh. (Latin, obturare = close, obscure) (The obturator nerve is considered by 73% of the members of the class of 2004 to be the "coolest-looking/prettiest nerve in the body". Other contenders were the sciatic nerve (20%) and the pudendal nerve (4%). This takes into account that only 21% of the class actually found the pudendal nerve.)
femoral nerve: from L2, L3, and L4. It runs inferiorly, along the border between the psoas major muscle and the iliacus muscle. It supplies motor innervation to the sartorius, rectus femoris, vastus lateralis, vastus intermedius, vastus medialis, and pectineus muscles, while providing sensory innervation to the skin of anterior thigh.
15. Describe the four common locations of porto-caval anastomosis. (N320 or TG 5-28)The white rami communicantes are only found as low as the L2 or L3 level. Inferior to that there are no sympathetic neuron cell bodies in the spinal cord, and are therefore no sympathetic fibers emerging from the cord into the spinal nerves. Since the white rami communicantes conduct fibers from the spinal nerve to the ganglia, they are unnecessary below L2 or L3. But, there are sympathetic fibers in the chain that have traveled from points superior, so there are gray rami communicantes, conducting fibers from the ganglia back onto the spinal nerve, along the chain's entire length.
There are four sites of porto-caval anastomosis described: distal esophageal veins, rectal venous plexus, paraumbilical veins, and posterior abdominal wall veins. These usually appear in roughly this order when portal hypertension, usually due to liver cirrhosis, causes pressure within the portal veins to increase because it has difficulty in passing through the liver sinusoids. The portal venous blood then finds alternate routes back into the caval venous system, bypassing the liver. In rough order of appearance in the progression of this condition:
distal esophageal veins: the thoracic esophagus drains to the azygos system of veins in the chest, while tributaries to the left gastric vein drain the distal esophagus ultimately into the portal vein. Retrograde passage of blood from the portal vein into these distal esophageal veins causes esophageal varicies, enlarged veins within the walls of the esophagus. If these rupture, the blood will be digested and produce black feces.
rectal venous plexus: the superior rectal vein drains the rectum into the inferior mesenteric vein and ultimately the portal vein, while the distal rectum and anal canal drain into the middle and inferior rectal veins, which drain into the internal iliac vein and ultimately into the inferior vena cava. It is commonly thought that retrograde flow of blood down the superior rectal tributaries engorge the veins in the anal columns and cause internal hemorrhoids. However, it has recently been shown that it is more accurate to describe these enlarged veins as within the rectal venous plexus within the walls of the rectum.
paraumbilical veins: very small veins called paraumbilical veins lie within the falciform ligament and drain into the portal vein within the liver. The paraumbilical veins have connections to veins draining the anterior abdominal wall, and retrograde blood in the paraumbilical veins will enlarge the anterior abdominal wall veins. The superficial veins of the anterior abdominal wall will be most visible, of course, and their engorgement, radiating from the umbilicus, is called caput medusa (after Medusa, the woman with the snake hair-do).
posterior abdominal wall veins: given enough back-pressure within the portal venous system, blood enlarges all of the tributaries into the portal system. The portal tributaries of the secondarily retroperitoneal organs (duodenum, pancreas, ascending and descending colon) can form anastomoses with veins of the posterior abdominal wall, the lumbar veins, that ultimately drain into the inferior vena cava usually.
Cultural enrichment: Check out these sections from the 1918 version of Gray's Anatomy of the Human Body! Some of the terms are (of course) out-of-date, but the illustrations are timeless.
Questions and Answers:
15. What is the vertebral level of an imaginary horizontal line drawn between the right and left iliac crests? (N 248 or TG 5-03)The line between the iliac crests is at the level of L4.16. What are the structures that enter and leave the kidney along the medial border and can be elevated with it? (N 334A, 334B,332 or TG 5-31)The renal veins, renal arteries, and the ureters enter and leave the kidney along the medial border and can be elevated with it.17. What are the anterior visceral relations of the kidneys? (N 329 or TG 5-31,342A, 342B,349 or TG 5-42) (See #1 above)18. What are the differences between the left and right renal veins? (N 332 or TG 5-31) (See #3 above)
- Left kidney: pancreas, stomach, large intestine, small intestine, spleen
- Right kidney: liver, large intestine, small intestine
The left renal vein is longer than the right renal vein since the inferior vena cava is on the right side of the body. There are also differences in the veins connecting to the renal veins, but this will be addressed later.19. How is the left renal vein related to the aorta, the superior mesenteric artery, and the left renal artery? (N 332 or TG 5-31)The left renal vein crosses anterior to the aorta and posterior to the superior mesenteric at a level just below the branch point of the superior mesenteric from the aorta. It runs anterior to the left renal artery.20. Where on the aorta are the origins of the renal arteries? (N 264 or TG 5-34,332 or TG 5-31)The renal arteries originate from the aorta approximately an inch below the celiac trunk, slightly inferior to the origin of the superior mesenteric artery. This is the upper L2 vertebral level.21. What is the developmental significance of the supernumerary (extra) renal arteries? (N 333)The kidneys develop within the pelvis and then ascend to their adult levels. As they travel up the posterior abdominal wall, the arterial supply actually remodels itself, to achieve a higher origin from the aorta. Supernumerary renal arteries are remnants of the earlier blood supply, and consequently they most commonly enter the inferior pole of the kidney. (See #3 above.)22. Describe the level of origin, variations, course, relations, and branches of the gonadal arteries and veins. (N 341 or TG 5-30,400, 401)The gonadal arteries originate from the anterior aspect of the aorta, below the renal arteries, at the lower L2 vertebral level. They have ureteric branches and descend obliquely (crossing over the ureters) either to the ovaries (as "ovarian arteries") or the deep inguinal canal (as "testicular arteries"). The gonadal veins follow the same path back from the respective organs, but end differently. The right gonadal vein drains into the inferior vena cava at the same level as the right gonadal artery originates from the aorta, and the left gonadal vein drains into the left renal vein.23. What is the relationship of the ureter to the gonadal vessels, the left colic vessels, and the root of the mesentery? (N 340,341,401 or TG 5-30, 5-30)The ureter passes posterior to the gonadal vessels, the left colic vessels, and the root of mesentery.24. What is the relationship between the renal artery, the renal vein, and the renal pelvis at the hilum of the kidney? (N 334A, 334B,335 or TG 5-32)The renal vein is anterior to the renal artery and pelvis. The renal artery mainly is anterior to the renal pelvis but a few of the branches enter the kidney posterior to the pelvis.25. What are the differences between the right and left suprarenal glands in terms of shape and relationship to the kidney? (N 332,341 or TG 5-31, 5-30)Both glands lie on top of the kidney and slightly medially. The right suprarenal gland is triangular and smaller than the left gland. The left gland is semilunar in shape.26. What is the relationship of the right suprarenal gland to the inferior vena cava? (N 341 or TG 5-30)The right gland makes contact medially with the inferior vena cava.27. Besides the inferior phrenic vein and the suprarenal vein, what other veins drain into the left renal vein? (N 332,341 or TG 5-31, 5-30)The left gonadal vein drains into the left renal vein, and the left 2nd lumbar vein drains into its posterior aspect. (See #19)28. Where are the postganglionic neurons of the suprarenal glands located? (N 348 or TG 5-39)The suprarenal medulla is directly innervated by preganglionic sympathetic fibers, causing a systemic sympathetic response. (The suprarenal (adrenal) medulla is modified nerve tissue. Activation of it causes the release of norepinephrine and/or epinephrine, which enter the blood stream and cause the systemic response.) However, postganglionic neurons from the celiac ganglion reach the cortical tissue of the suprarenal glands to innervate the suprarenal blood vessels.29. What is the relationship of the median, medial, and lateral arcuate ligaments to the aorta, psoas major, and quadratus lumborum muscles? (N 263 or TG 5-33)The lateral arcuate ligament passes across the quadratus lumborum muscle, the medial arcuate ligament over the psoas major, and a median arcuate ligament is related to neither but forms the aortic hiatus by uniting the two crura.30. How are the medial and lateral arcuate ligaments formed and what are their bony attachments? (N 195,263 or TG 5-33)The medial arcuate ligament goes from the body of the first or second lumbar vertebra to the transverse process of the first lumbar vertebra. The lateral arcuate ligament goes from the transverse process of L1 to the tip of the 12th rib.31. What is the lumbocostal triangle and what is its significance? (N 189,263 or TG 5-33)The lumbocostal triangle is an area of the diaphragm superior to the lateral arcuate ligament. Here, the diaphragmatic muscle is deficient and the triangle is closed primarily by the inferior and superior fascia of the diaphragm. It is a significant area for hernias.32. Are there other innervations, besides the phrenic nerves, to the inferior surface of the diaphragm? (N 195,193 or TG 4-29)The phrenic nerve is the only motor nerve of the diaphragm.33. What are the differences in the formation and the structures transmitted by each diaphragmatic hiatus? What are the average vertebral levels of each? (See #6 above) (N 189,263,267 or TG 5-33, 5-38)34. Concerning the abdominal aorta, note the point and level of bifurcation, course, relations, branches, and vertebral levels of each. (N 264 or TG 5-34)
- aortic hiatus: formed by the median arcuate arch, or the medial tendinous margins of the crura, at the T12 vertebral level. The aorta and the thoracic duct pass through this hiatus.
- esophageal hiatus: formed by the right crus at the T10 vertebral level. The esophagus and the vagal trunks pass through this opening.
- caval hiatus: an opening in the central tendon at the T8 vertebral level that conducts the inferior vena cava.
35. How do the lumbar segmental arteries and the median sacral artery compare with the thoracic segmental vessels? (N 264 or TG 5-34)See #7 above.
36. Describe the relations of the inferior vena cava to the aorta and viscera throughout the abdomen. (N 265,273,274,349 or TG 5-30 5-34, 5-42)Lumbar arteries 1-4 are segmental in a similar fashion to the posterior intercostal arteries. The median sacral artery is a poor attempt to provide a 5th lumbar artery - it is a fairly small vessel. The 5th lumbar artery is replaced by the iliolumbar artery from the internal iliac artery.
37. Do all lumbar segmental veins terminate in the vena cava? (N 332 or TG 5-31)The inferior vena cava runs lateral to the aorta on the right side. It is slightly more anterior as well until the level of L4. Below that, the aorta becomes more anterior and the right common iliac artery crosses over the inferior vena cava and the common iliac vein. The inferior vena cava passes behind the liver, stomach, small intestine, and pancreas.
38. What is the significance of the location of the celiac branches of the posterior vagal trunk as they join the celiac plexus? (N 318,319, 320 or TG 5-39)No, the left second lumbar often empties into the left renal vein.
39. Is there a superior mesenteric ganglion around the superior mesenteric artery? (N 318 or TG 5-39)The significance of this branch of the vagus is that it distributes to the organs supplied by the celiac and superior mesenteric arteries.
40. Is there an inferior mesenteric plexus or ganglia around the inferior mesenteric artery? (N 318 or TG 5-39)Yes, but it is often fused with the celiac ganglia.
41. How does the thoracic sympathetic trunk get into the abdomen? (N 195)Yes, but the ganglion may be small or indistinguishable.
42. How many splanchnic nerves are there? What part of the preaortic plexus do they join? (N 318 or TG 5-39)The sympathetic trunk passes beneath the medial arcuate ligament on each side.
43. Organize the autonomic distribution to the abdominal viscera. How is this distribution completed from the structures you have seen today? (N 318, 319, 322, 323 or TG 5-39)See #8 above.
See #8, 9, and 10 above.
An additional point is this: sympathetic nerves synapsing in the the celiac ganglion innervate the foregut, sympathetic nerves synapsing in the superior mesenteric ganglion innervate the midgut, and sympathetic nerves synapsing in the the inferior mesenteric innervate the hindgut.
44. What is the source of the afferent drainage of the lumbar lymph trunks and the intestinal lymph trunk? (N 546, 266 or TG 5-37)
45. How do you distinguish between the white and gray rami communicantes? (N 160, 267 or TG 5-38)The lumbar trunks drain the lower limbs, pelvis, and abdominal wall structures. The intestinal trunk drains the gastrointestinal tract. It usually unites with the left lumbar trunk before the two lumbar trunks unite to form the cisterna chyli or, if no dilatation occurs, the thoracic duct.
White rami communicantes are generally more lateral going into the ventral primary ramus. Also, any rami below the L2 level can only be gray, since the thoracolumbar outflow of sympathetics from the spinal cord only exists between T1 and L2.46. How many white rami are there? Why? (N 160 or TG 8-02C,8-02D)47. Note the relationship between the quadratus lumborum and iliacus muscles. (N 263 or TG 5-33)In the entire body, there are 14 pairs of white rami and 31 pairs of gray rami. Each spinal nerve between T1 and L2 has a white ramus communicans, in addition to the gray ramus communicantes that each of the 31 pairs of spinal nerves receives. Within the abdomen, you will only find white rami at L1 and L2 levels, while gray rami are found on every spinal nerve, at every vertebral level.
Both have origins from the iliac crest, with quadratus lumborum inserting superiorly to the 12th rib while iliacus inserts inferiorly on the femur.48. To what group of muscles does the iliopsoas muscle belong? (N 263 or TG 5-33)49. Organize the actions of all muscles of the thigh.It belongs to the flexor group, which flex the thigh.
See the thigh and gluteal lab tables.50. Medial to the external iliac vein is the femoral ring. What ligaments surround it on three sides? (N 546, 251 or TG 5-05)The inguinal ligament lies anteriorly, the lacunar ligament marks the medial boundary (along with the lateral edge of the falx inguinalis), and the pectineal ligament lies posteriorly.51. Do you find a deep inguinal node within the femoral ring? (N 546 or TG 5-37)You should. There are usually about three deep inguinal nodes, and the one the lies in the femoral ring is know as the "node of Cloquet".