|
|
|
||||||||||||
Dissector Answers - Axilla, Posterior Shoulder, & Arm |
|||||||||||||
Learning Objectives:
Upon completion of this session, the student will be able to:
- Describe the lymphatic drainage of the upper limb and the major lymphatic node groups of the axilla.
- Recall the concept of the axilla as a space, its boundaries and its contents.
- Illustrate or describe the brachial plexus, including its parts, the nerves arising from it, and their specific origins and areas of distribution.
- Predict the functional and cutaneous loss that might result in the back, posterior shoulder, pectoral region, or cutaneous upper limb, given an injury to a specific site in the brachial plexus.
- Predict where the brachial plexus might be injured, given a functional or cutaneous loss in the back, posterior shoulder, pectoral region or cutaneous upper limb.
- Identify or describe the axillary artery and vein, their major branches, and their relationships to each other, the brachial plexus, and the pectoralis minor muscle.
- Identify the posterior shoulder muscles and associated rotator cuff muscles. Give their general functions and nerve supply.
- Identify and demonstrate the regional blood supply of the posterior shoulder.
- Identify prominent features of the humerus, cubital fossa and associated prominences of the scapula, radius and ulna as given in the lab manual.
- Identify the contents of each of the three compartments of the arm and the functional significance of the included muscles.
- Correlate any fractures of the humerus with functional disruptions of associated muscular and neurovascular structures.
- Describe the movements of the shoulder and elbow joints.
- Identify spatial relationships of all associated muscular and neurovascular structures within the cubital fossa.
Learning Objectives and Explanations:
1. Describe the lymphatic drainage of the upper limb and the major lymphatic node groups of the axilla. (W&B 106-107, 123, N184, N483, TG2-11)2. Recall the concept of the axilla as a space, its boundaries and its contents. (W&B 114-115, N181, TG2-11, TG2-12, TG2-13)As a general rule, the superficial lymphatic drainage of the upper limb follows the superficial venous drainage. Most of the lymph ends up in the lateral and central axillary lymph nodes, with some of it passing through the cubital lymph nodes along the way. Some of the lymph from the posterior surface of the upper limb travels in vessels that accompany the cephalic vein, piercing the clavipectoral fascia to end in the apical axillary lymph node. The deep lymphatic vessels of the upper limb accompany the major arteries to also end in the lateral and central axillary lymph nodes.
So what about these axillary lymph nodes? They are extremely important clinically, since they drain the major portion of the breast. These lymph nodes are carefully palpated during any thorough breast exam. There are five groups:
- anterior axillary (pectoral) lymph nodes: along the lower border of the pectoralis major muscle
- lateral axillary (humeral) lymph nodes: distal along the axillary vein
- posterior axillary (subscapular) lymph nodes: along the subscapular vein and its tributaries
- central axillary lymph nodes: centrally located along the axillary vein, deep to the pectoralis minor insertion
- apical axillary lymph node(s): at the apex of the axilla, receiving lymph from all other groups
3. Illustrate or describe the brachial plexus, including its parts, the nerves arising from it, and their specific origins and areas of distribution. (W&B 119-123, 708-714, N429, N430, TG2-13, TG2-14)The axillary space is shaped like a truncated pyramid. Its boundaries are:
- anterior wall: pectoralis major and minor muscles. The lateral border of pectoralis major muscle forms the anterior axillary fold.
- posterior wall: scapula, subscapularis muscle, teres major muscle, and latissimus dorsi muscle. The teres major muscle combines with latissimus dorsi muscle to form the posterior axillary fold.
- medial wall: serratus anterior muscle
- lateral wall: the floor of the intertubercular groove of the humerus.
4. Predict the functional and cutaneous loss that might result in the back, posterior shoulder, pectoral region, or cutaneous upper limb, given an injury to a specific site in the brachial plexus. (W&B 185-186, N430, TG2-14)
Images from "Anatomy of the Human Body" by Henry Gray are provided by:
The brachial plexus consists of roots, trunks, divisions, cords, and branches. There is a classic mnemonic to help with this one: Robert Taylor Drinks Cold Beer. The roots are mostly derived from the ventral primary rami of C5 to T1. Three trunks, the superior, middle and inferior trunks, are derived from those roots (C5-C6, C7, and C8-T1 respectively). Each trunk divides into an anterior and posterior division. The posterior divisions of all three trunks unite to form the posterior cord. The anterior divisions of the superior and middle trunks unite to form the lateral cord. Finally, the anterior division of the inferior trunk forms the medial cord. (The medial aspect of your arm when it is in the anatomical position is also the inferior aspect when you stick your arm straight out, or, for that matter, when you are an embryo and your arm is 2mm long. In the same way, lateral is superior.) These cords then terminate as branches that supply the skin and muscles of the upper limb.
For the rest, we will rely on the tables:
Nerve Source Branches Motor Sensory nerves from the roots: dorsal scapular brachial plexus (C5) rhomboid major & minor; levator scapulae long thoracic brachial plexus (C5-C7) serratus anterior nerves from the trunks: to subclavius superior trunk of brachial plexus subclavius suprascapular superior trunk of brachial plexus (C5-C6) supraspinatus, infraspinatus terminal branches (i.e., from the cords): lateral pectoral lateral cord of brachial plexus pectoralis major musculocutaneous lateral cord of brachial plexus (C5,6) lateral antebrachial cutaneous coracobrachialis, biceps brachii, brachialis skin of lateral side of forearm medial pectoral medial cord of the brachial plexus pectoralis minor & major medial brachial cutaneous medial cord of brachial plexus skin of the medial side of the arm medial antebrachial cutaneous medial cord of brachial plexus skin of medial side of forearm median lateral & medial cords of brachial plexus anterior interosseous, palmar br., recurrent (motor) Br, common palmar digital ns. (1st-3rd) pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, flexor digitorum profundus (radial half), flexor pollicis longus, pronator quadratus, abductor pollicis brevis, flexor pollicis brevis, opponens pollicis, radial 2 lumbricals skin of radial half of palm & palmar side of radial 3 1/2 digits (and nail bed for these digits) ulnar medial cord of the brachial plexus palmar cutaneous Br, dorsal Br, superficial & deep Br flexor carpi ulnaris, flexor digitorum profundus (ulnar half), abductor digiti minimi, flexor digiti minimi brevis, opponens digiti minimi, ulnar 2 lumbricals, palmar & dorsal interossei skin of medial side of wrist & hand & ulnar 1 1/2 digits upper subscapular posterior cord of brachial plexus subscapularis thoracodorsal (middle subscapular) posterior cord of brachial plexus latissimus dorsi lower subscapular posterior cord of brachial plexus subscapularis, teres major radial posterior cord of brachial plexus posterior brachial cutaneous, inferior lateral brachial cutaneous, posterior antebrachial cutaneous, superficial & deep br triceps brachii, anconeus, brachioradialis, extensor carpi ulnaris, extensor carpi radialis longus & brevis, extensor digitorum, extensor digiti minimi, supinator, abductor pollicis longus, extensor pollicis longus & brevis, extensor indicis skin of posterior arm, forearm & hand axillary posterior cord of brachial plexus superior lateral brachial cutaneous n. deltoid, teres minor skin of upper lateral arm 5. Predict where the brachial plexus might be injured, given a functional or cutaneous loss in the back, posterior shoulder, pectoral region or cutaneous upper limb. (N430, TG2-14)Symptoms of brachial plexus injury may include a limp or paralyzed arm, lack of muscle control in the arm, hand, or wrist, and lack of feeling or sensation in the arm or hand. Although injuries can occur at any time, many brachial plexus injuries happen during birth: the baby's shoulders may become impacted during the birth process causing the brachial plexus nerves to stretch or tear. There are four types of brachial plexus injuries: avulsion, the most severe type, in which the nerve is torn from the spine; rupture, in which the nerve is torn but not at the spinal attachment; neuroma, in which the nerve has tried to heal itself but scar tissue has grown around the injury, putting pressure on the injured nerve and preventing the nerve from conducting signals to the muscles; and neuropraxia or stretch, in which the nerve has been damaged but not torn. Neuropraxia is the most common type of brachial plexus injury.
These injuries usually occur at the roots. The upper roots of the brachial plexus supply the more proximal muscles, while the lower roots supply the more distal. The segmental innervation of the skin does not correlate with the supply of the muscles beneath.
Injury to the upper roots, C5 and C6, are the most common type. This results in Erb-Duchenne Palsy, or "Waiter's Tip". It affects the suprascapular nerve especially and frequently also involves the musculocutaneous and axillary nerves, which results in paralysis of the rotator cuff muscles, in addition to the biceps, brachialis, coracobrachialis, and deltoid muscles. Subscapularis may also be affected. The upper limb hangs limply, medially rotated by unopposed pectoralis major, latissimus dorsi, and teres major muscles and pronated due to loss of biceps.
Injury to the lower roots, C8 and T1, results in Klumpke's Palsy. The ulnar and median nerves are affected, paralyzing all of the intrinsic muscles of hand. Patients present with a "clawed hand" due to hyperextension of MP joints and flexion of digits by forearm flexors unopposed by interossei.
As for related cutaneous losses, check out a diagram of the cutaneous nerves of the upper limb.
6. Identify or describe the axillary artery and vein, their major branches, and their relationships to each other, the brachial plexus, and the pectoralis minor muscle. (W&B 115-119, N427, N429, N256, TG2-19, TG2-15A, TG2-15B)If you know where the nerves go and what they innervate, then you will be able to work backwards:
- "Hey Doc, my shoulder blade is sticking out of my back like an angel's wing."
- "Well, Hank, you must have injured your long thoracic nerve."
- "Yeah, come to think of it, I fell off my bike and stretched my neck to the right the other day."
The possibilities are numerous. See #3 and #4 above.
7. Identify and demonstrate the posterior shoulder muscles and associated rotator cuff muscles. Give their general functions and nerve supply. (N425, N426, N427, TG2-08A, TG2-08B, TG2-16A, TG2-16B, TG2-16C)
Images from "Anatomy of the Human Body" by Henry Gray are provided by:
The axillary artery is the second portion of the upper limb's main arterial stem. (This arterial stem changes names regionally, even though it is all really the same vessel. It is like the external iliac, femoral, and popliteal arteries in the lower limb.) The axillary artery is defined to be the distal continuation of the subclavian artery, after that artery passes over the first rib. It continues to the inferior border of teres major where its name changes to the brachial artery.
The axillary artery is divided into three parts, numbered proximally to distally as parts 1, 2 and 3. Each part is defined in relation to the pectoralis minor muscle, which, by definition, covers the 2nd portion of the axillary artery. (The portion proximal to pectoralis minor is therefore the1st part of the axillary artery, while the portion distal to pectoralis minor is the 3rd portion of the axillary artery.
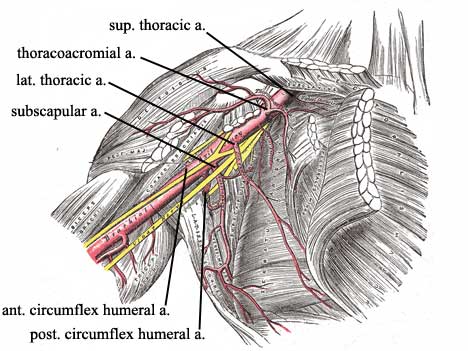
The 1st part has one branch, the superior thoracic artery, which supplies the intercostal muscles of the 1st and 2nd intercostal spaces and the upper portion of serratus anterior muscle.
The 2nd part has two branches, the thoracoacromial and lateral thoracic arteries. The thoracoacromial artery is a short trunk arising anteriorly and passing medial to the pectoralis minor muscle. It divides into four branches distributing according to their regional names: acromial, deltoid, pectoral and clavicular. The lateral thoracic artery is a variable artery that, in 65% of us, is a direct branch of the axillary artery, but can also arise from the thoracoacromial or subscapular arteries. It passes below the inferolateral border of pectoralis minor muscle to distribute most significantly to serratus anterior and the pectoral muscles.
The 3rd part has three branches. The subscapular artery is the largest branch of the axillary artery. It divides into the circumflex scapular and thoracodorsal branches three or four centimeters from its origin. The circumflex scapular artery passes through the triangular space and supplies the infraspinatous, subscapular, teres major, and teres minor muscles. It also anastomoses with the infraspinatous branch of the suprascapular artery in the infraspinatus fossa. The thoracodorsal artery is the principal supply to the latissimus dorsi muscle and is accompanied by the thoracodorsal nerve. The next branch of the 3rd part of the axillary artery is the anterior circumflex humeral artery. It runs anteriorly around the surgical neck of the humerus and anastomoses with the posterior circumflex humeral artery, which is the final branch of the 3rd part of the axillary artery. This is larger than its anterior partner, and passes through the quadrangular space with the axillary nerve.
As for the axillary vein, it begins as the union of the brachial veins with the basilic vein. It continues through the axilla, medial to the axillary artery, until it changes its name to the subclavian vein at the lateral border of the first rib. The axillary vein receives the cephalic vein and numerous other tributaries that roughly correspond to the branches of the axillary artery, though things are of course somewhat variable (See #15 below). (One thing to note is that the vein receives one or more thoracoepigastric veins, which represent anastomoses of veins from the superficial inguinal region with one or more axillary tributaries. This represents a possible route of collateral drainage if the inferior vena cava is obstructed for some reason.)
8. Identify and demonstrate the regional blood supply to the shoulder. (W&B 115-118, N426, N427, TG2-08B, TG2-09A)
Muscle Origin Insertion Action Innervation deltoid lateral one-third of clavicle, acromion, lower lip of the crest of the spine of the scapula deltoid tuberosity of the humerus abducts arm; anterior fibers flex & medially rotate arm; posterior fibers extend & laterally rotate arm axillary nerve (C5,6) from posterior cord of brachial plexus teres major dorsum of the inferior angle of scapula crest of lesser tubercle of humerus adducts arm, medially rotates arm, assists in arm extension lower subscapular nerve (C5,6) from the posterior cord of the brachial plexus
Rotator Cuff:
Muscle Origin Insertion Action Innervation supraspinatus supraspinatus fossa greater tubercle of humerus (highest facet) abduct arm (initiate abduction) suprascapular nerve (C5,6) from superior trunk of brachial plexus infraspinatus infraspinatus fossa greater tubercle of humerus (middle facet) laterally rotate arm suprascapular nerve teres minor upper 2/3 of the lateral border of the scapula greater tubercle of humerus (lowest facet) laterally rotates arm axillary subscapularis medial two-thirds of costal surface of scapula (subscapular fossa) lesser tubercle of humerus medially rotates arm; assists extension of arm upper and lower subscapular nerves (C5,6)
The rotator cuff is a musculotendinous cuff around the glenohumeral joint. To remember the muscles that participate in it, use the mnemonic "SITS": Supraspinatus, Infraspinatus, Teres minor, Subscapularis. The tendons of these muscles reinforce the articular capsule of this joint. Their main purpose is to hold the head of the humerus in the glenoid cavity during movement of the arm. (The rotator cuff's vulnerable aspect is that it does not effectively prevent dislocations of the shoulder if the arm is pulled straight down, since it is incomplete inferiorly. Otherwise, the most common way to damage the cuff is seen in the example of a hockey player who collides into a wall with her arm stuck straight out in front of her to absorb the shock.)The axillary artery is the primary source of blood to the region. (It continues as the brachial artery, which supplies the upper limb.) The artery proper, including all of its branches, will be given complete treatment with the axilla. For now, there are a few important concepts to begin thinking about.9. Identify prominent features of the humerus, cubital fossa and associated prominences of the scapula, radius and ulna as given in the lab manual. (N420, N421, N436, N439, TG2-03A, TG2-03B, TG2-04)
Two branches of the third part of the axillary artery are the anterior and the posterior circumflex humeral arteries. These form a circle of blood flow around the surgical neck of the humerus. The posterior is larger than the anterior, and accompanies the axillary nerve through the quadrangular space.
The important arteries that form anastomoses around the scapula are the dorsal scapular, suprascapular and subscapular, and, one of its branches, the circumflex scapular artery. A visual must be consulted to truly get the picture, however, the significance of the anastamoses of the shoulder is that if one of these arteries is occluded there are other routes through which the blood supply can reach the area, thereby avoiding ischemia. Also, surgical ligatures can be placed on the suprascapular, axillary or subscapular arteries without damaging the muscles of the shoulder.10. Identify the contents of each of the three compartments of the arm and the functional significance of the included muscles. (W&B 124-127, N184, N420, N421, N426, N429, N431, N433, N434, N435, N447, N473, N474, N475, N476, N477, N479, N480, TG2-17A, TG2-17B, TG2-18A, TG2-18B, TG2-19A, TG2-19B, TG2-20A, TG2-20B)The only prominent feature of the humerus that we are worried about here is the radial groove, which spirals around the posterior surface of the shaft of the humerus, containing the radial nerve and the deep brachial vessels. See the next session for prominent features of the bones of the forearm.
11. Correlate any fractures of the humerus with functional disruptions of associated muscular and neurovascular structures. (N426, N434, N477, TG2-19B, TG2-20B)The medial and lateral intermuscular septa divide the arm into an anterior (flexor) compartment and a posterior (extensor) compartment. Furthermore, the medial intermuscular septum consists of two laminae, and the space between them is the neurovascular compartment. The contents of each compartment are listed below:
anterior (flexor) compartment:
Muscle Origin Insertion Action Innervation biceps brachii short head: tip of coracoid process; long head: supraglenoid tubercule of scapula tuberosity of radius flexes forearm, flexes arm (long head), supinates musculocutaneous nerve (C5,6) brachialis anterior surface of lower one-half of humerus and intermuscular septa coronoid process of ulna flexes forearm musculocutaneous nerve (C5,6) coracobrachialis coracoid process of scapula medial humerus at mid-shaft flexes and adducts arm musculocutaneous nerve (C5,6)
posterior (extensor) compartment:
Muscle Origin Insertion Action Innervation triceps brachii long head: infraglenoid tubercle of scapula; lateral head: posterolateral humerus & lateral intermuscular septum; medial head: posteromedial surface of inferior 1/2 of humerus olecranon process of the ulna extends forearm; long head extends and adducts arm radial nerve anconeus lateral epicondyle lateral side of olecranon and upper one-fourth of ulna extends forearm nerve to anconeus from radial nerve
Neurovascular structure Source Branches Supply to: ulnar nerve medial cord of the brachial plexus palmar cutaneous Br, dorsal Br, superficial & deep Br motor: flexor carpi ulnaris, flexor digitorum profundus (ulnar half), abductor digiti minimi, flexor digiti minimi brevis, opponens digiti minimi, ulnar 2 lumbricals, palmar & dorsal interossei
sensory: skin of medial side of wrist & hand & ulnar 1 1/2 digits
neurovascular compartment:
Neurovascular structure Source Branches Supply to: brachial artery axillary (continuation distal to teres major m.) deep brachial, sup. ulnar collateral, nutrient, inf. ulnar collateral; terminal branches are the radial & ulnar arm, forearm & hand median nerve lateral & medial cords of brachial plexus anterior interosseous, palmar br, recurrent (motor) br, common palmar digital nn (1st-3rd) motor: pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, flexor digitorum profundus (radial half), flexor pollicis longus, pronator quadratus, abductor pollicis brevis, flexor pollicis brevis, opponens pollicis, radial 2 lumbricals
sensory: skin of radial half of palm & palmar side of radial 3 1/2 digits (and nail bed for these digits)The compartment also contains the basilic vein and several brachial veins.
12. Describe the movements of the shoulder and elbow joints.The humerus can break just about anywhere along its length. The three most common places, due to relative weakness, are the surgical neck, the distal end of the middle 1/3 of the bone, and the supracondylar region. With surgical neck fractures, laceration of the axillary nerve and one or both circumflex humeral arteries could cause a significant problem. In the case of a fracture more distal along the shaft, the structure most in danger is the radial nerve, which is wrapping around the bone in the radial groove. According to Wheeless's Textbook of Orthopaedics, radial nerve palsy of some degree occurs with 18% of humeral shaft fractures.
13. Identify spatial relationships of all associated muscular and neurovascular structures within the cubital fossa. (W&B 132-134, N447, N479, TG2-23, TG2-24)The shoulder joint is a ball and socket joint. Movements there include flexion, extension, abduction, adduction, and circumduction, as well as medial and lateral rotation of the arm. The elbow joint is a hinge, permitting only flexion and extension.
The floor of the cubital fossa is the brachialis and supinator muscles, so all of the contents of the space lie superficial to those two structures. The tendon of the biceps brachii runs through the middle of the cubital fossa. Medial to it we find the brachial artery (which splits into radial and ulnar arteries near the inferior border of the cubital fossa). The median nerve lies medial to the brachial artery as they both enter the forearm. More superficially we find the median cubital vein, the lateral antebrachial cutaneous nerve, and branches of the medial antebrachial cutaneous nerve.
Cultural enrichment: Check out these sections from the 1918 version of Gray's Anatomy of the Human Body! Some of the terms are (of course) out-of-date, but the illustrations are timeless. The Anterior Divisions (nerves) - The Veins of the Upper Extremity and Thorax - The Axillary Artery - The Brachial Artery - The Muscles and Fascia¾ of the Shoulder - The Muscles and Fascia of the Arm - Surface Anatomy of the Upper Extremity - Surface Markings of the Upper Extremity
Questions and Answers:
14. Define the boundaries of the axillary space.See #2 above. (N181, TG2-12)15. How is the axillary vein formed?16. Is the axillary vein a single, paired or plexiform vein?It's formed by the union of the brachial veins (which accompany the brachial artery) and the basilic vein at the inferior border of teres major. (N184, TG2-53)
17. Do the tributaries of the axillary vein correspond to the axillary arterial branches?The axillary is normally a single vein.
18. Are the axillary vein's tributaries paired?Yes, with the exception of the thoracoacromial vein, whose branches join the axillary vein independently and the cephalic vein which has no corresponding artery. (N427, N256, TG2-19, TG2-53)
19. Can you see any valves in the veins?Some, such as the brachial veins, are paired. Others, such as cephalic vein, are not. (N184, TG2-53)
20. Establish relationships of axillary artery and vein within the axilla.There are valves within the axillary vein, and valves are also located in tributaries where they join the axillary vein.
21. Do you see a separate medial brachial cutaneous n.?At its source, the vein lies on the medial side of the artery, partly overlapping it. Thereafter, in the upper part of the axilla, the vein lies anterior and inferior to the artery. (N429, N479, TG2-11)
22. What artery accompanies the axillary nerve?The medial brachial cutaneous nerve is much smaller than the medial antebrachial cutaneous nerve, and, once the skin of the axilla is removed, it may be difficult to find. It branches from the medial cord, just proximal to the medial antebrachial cutaneous nerve. It may make a nerve anastomosis with the intercostobrachial nerve. (TG2-13)
23. What does lower subscapular nerve accompany?The posterior circumflex humeral artery, a branch of the 3rd part of the axillary artery, accompanies the axillary nerve through the quadrangular space. (N426, N432, TG2-18, TG2-19, TG2-20)
24. Note how the three cords of the brachial plexus are derived from the trunks.Lower subscapular nerve accompanies circumflex scapular artery into the triangular space. (N426, TG2-13, TG2-15)
25. Note course, relations and parts of the axillary artery.26. Note the area of distribution of the axillary artery's branches as well as any accompanying nerves:27. What is the source of the long thoracic nerve and what is "winged scapula"?28. Does the supraspinatus muscle use the fascia spanning the area from the spine to the superior border of the scapula?The long thoracic nerve arises from the anterior rami of C5-C7. Winged scapula is a condition in which the scapula protrudes from the back because it is not held in place by the counterbalancing forces of the serratus anterior and trapezius muscles. It results from injury to the long thoracic nerve. See #5 above. (N191, N429, TG2-14)
Yes, it arises from the dense fascia covering the muscle. It arises from the medial 2/3 of the walls of the fossa.29. Does the subacromial bursa continue laterally deep to the deltoid muscle? Significance?The subacromial bursa is a "synovial bursa" situated directly under the deltoid muscle, between it and the supraspinatus tendon and the joint capsule. It has an extension which runs deep to the acromion and the coracoacromial ligament. The bursa facilitates the movement of the deltoid muscle over the joint capsule and tendons. (N423, TG2-42)30. To how much of the supraspinous fossa does the supraspinatus muscle attach?Although the supraspinatus muscle fills the supraspinous fossa, it arises primarily from the medial aspects of this fossa. (N426, TG2-06)31. How are the suprascapular artery, vein, and nerve related to the scapular notch?The suprascapular notch is bridged by the superior transverse scapular ligament. The suprascapular nerve passes under the ligament. The suprascapular artery and vein pass over it. (The navy goes under the bridge, the army goes over.) (N426,N427, TG2-08)32. How much of the fossa is used for the infraspinatus muscle attachment?The infraspinatus muscle arises from the whole of the infraspinatus fossa except its lateral 1/4, and from the overlying infraspinatus fascia and the intermuscular septa. (N425, N426, TG2-06)33. Trace the nerve, artery, and vein from the supraspinatus to the infraspinatus fossa around the notch of the neck of the scapula. Does the artery terminate in the infraspinatus muscle?Semantically, the artery comes to an end, but really it enters into the anastomoses of the shoulder region, specifically with the circumflex scapular artery. (N426,N427, TG2-08)34. Is the teres minor muscle separated or fused with the lateral border of the infraspinatus?The teres minor muscle is often totally fused with the lateral border of the infraspinatus muscle. (N425, TG2-08)35. For the question about the rotator cuff, see the treatment of the theme above under the lab objectives.See #7 above. (N421,N426,N429,N430, TG2-16Aa>, TG2-16Ba>, TG2-16C)36. What are the boundaries of the quadrangular space? What does it transmit?The borders of the quadrangular space are:37. Find the circumflex scapular artery in the triangular space. Is there an open anastomosis between it and the suprascapular artery?The space transmits the axillary nerve and the posterior circumflex humeral artery. (N426, TG2-08)
- inferior: teres major muscle
- lateral: humerus
- superior: teres minor muscle
- medial: the long head of the triceps muscle.
There is usually an open anastomosis between the circumflex scapular artery and the suprascapular artery. (N426,N427, TG2-08)38. Identify the circumflex scapular artery. What does it supply? Does it anastomose with the suprascapular artery?The triangular space transmits the circumflex scapular artery. This vessel feeds the muscles of the dorsum of the scapula and participates in the anastomoses described above. It certainly does anastomose with the suprascapular artery. (N426,N427, TG2-08)39. Do muscles use the intermuscular septa as attachments?40. Where do branches of the musculocutaneous nerve enter anterior compartment muscles?The lateral and medial heads of triceps brachii and brachialis all use intermuscular septae as part of their origins.
41. How does the musculocutaneous nerve terminate, where does it change its name, and does it have any accompanying arteries?The musculocutaneous nerve is the continuation of the lateral cord of the brachial plexus after that cord's contribution to the median nerve. The musculocutaneous nerve gives off branches to the coracobrachialis as it pierces that muscle. It continues downward in the interval between the brachialis muscle and biceps brachii muscle, giving branches to each. (TG2-17)
42. How is the neurovascular compartment of the arm formed?The musculocutaneous nerve terminates by piercing the brachial fascia lateral to the biceps tendon a short distance above the elbow. It continues as the lateral antebrachial cutaneous nerve. It has no accompanying arteries. (N474, TG2-17)
43. What are the relations and branches of the median nerve in the arm?The medial intermuscular septum is divided into two laminae, which, with the overlying brachial fascia, form the neurovascular compartment. (N435)
44. Where does the ulnar nerve leave the neurovascular compartment?The median nerve has no muscular branches in the arm. Initially it rests atop the brachial artery in the neurovascular compartment, then comes to lie anterolateral to the brachial artery and is overlapped laterally by the coracobrachialis muscle. The nerve eventually becomes medial to the brachial artery, crossing over it at the midarm level. (N435, N475, TG2-17)
45. Does the ulnar nerve have any branches in the arm?At approximately mid-arm, the ulnar nerve pierces the posterior layer of the intermuscular septum to enter the posterior compartment. (N433, N435, N473, N476)
46. Is the ulnar nerve accompanied by any vessels in the arm? (N434)No, it does not.
47. Is the brachial vein paired? How is it formed? What does it continue as? Where does the basilic vein join it?The superior ulnar collateral artery, one of the arteries of the elbow collateral circulation, accompanies ulnar nerve posterior to the medial epicondyle.
48. What are the collateral branches of the brachial artery around the elbow?The brachial vein is a paired set accompanying the brachial artery. It is formed at the elbow by the union of venae comitantes of the radial and ulnar arteries. It continues as the single axillary vein, after the two veins join at about the lower border of teres major muscle. (N434, N256, TG2-53)
49. Locate the brachial artery and median nerve. What are their relative positions?The brachial artery gives off two collateral branches for the elbow anastomosis: the superior ulnar collateral artery at mid-arm, that accompanies the ulnar nerve, and the inferior ulnar collateral artery, that passes anterior to the medial epicondyle. (N434, TG2-46)
50. Where does the brachial artery divide?Remember TAN - in the cubital fossa, the biceps Tendon lies lateral, the brachial Artery is intermediate, and the median Nerve is most medial. (N433, TG2-17)
51. What happens to the median nerve?Within the cubital fossa, the brachial artery divides into the radial and ulnar arteries. (N447, TG2-24)
52. Separate the brachialis from the brachioradialis muscle along the intermuscular septum between them and identify the radial nerve. Is it accompanied by vessels? What are they?The median nerve passes into the forearm through the two heads of pronator teres. (N448, N475, TG2-24, TG2-25)
53. What structures in the superficial fascia overlie the cubital fossa? What is their importance? Danger?The radial nerve is accompanied above the elbow by the radial collateral artery, a terminal branch of the deep brachial artery. Below the elbow, radial nerve is accompanied by the radial recurrent artery, that anastomoses with the radial collateral. (N447, N448, TG2-24)
54. What nerve is given off to the forearm by the radial nerve as it enters the anterior compartment?Branches of the medial antebrachial cutaneous nerve cross the medial portion of the cubital fossa, while the lateral antebrachial cutaneous nerve emerges from beneath the biceps on the lateral side of the cubital fossa. The median cubital vein also crosses the fossa obliquely, shunting blood from the cephalic vein up to join the basilic vein. This is a common site for phlebotomy, and cutaneous nerves may be in danger here. (N480, TG2-02)
As the radial nerve pierces the lateral intermuscular septum it gives off the posterior antebrachial cutaneous nerve, which supplies the skin of the back of the forearm. (N477, TG2-18)